Life-Supporting Treatment Limitations in Patients Who Die Within 48 Hours After ICU Admission: A French, Multicenter, Observational, Exploratory Study.
Aurélie Nouvel, Pierre Leprovost, Charlotte Larrat, Xavier Valette, Isabelle Vinatier, Agathe Delbove, David Schnell, Anne Renault, Pauline Cailliez, Maud Jonas, Pauline Guillot, Anthony Lemeur, Jean Reignier, Théophile Lancrey-Javal, Reyes Munoz Calahorro, Soline Bobet, Gauthier Blonz
{"title":"Life-Supporting Treatment Limitations in Patients Who Die Within 48 Hours After ICU Admission: A French, Multicenter, Observational, Exploratory Study.","authors":"Aurélie Nouvel, Pierre Leprovost, Charlotte Larrat, Xavier Valette, Isabelle Vinatier, Agathe Delbove, David Schnell, Anne Renault, Pauline Cailliez, Maud Jonas, Pauline Guillot, Anthony Lemeur, Jean Reignier, Théophile Lancrey-Javal, Reyes Munoz Calahorro, Soline Bobet, Gauthier Blonz","doi":"10.1097/CCE.0000000000001300","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>The occurrence of death shortly after ICU admission raises concerns about the appropriateness of providing intensive care to frail patients-many of whom are subsequently subject to decisions to limit life-supporting treatment limitation (LST-L). The proportion of patients who die early and are affected by such limitations remains unknown.</p><p><strong>Objectives: </strong>The primary objective was to determine the proportion of patients with a decision of LST-L among patients who died within 48 hours after ICU admission. We also conducted analyses to identify variables associated with LST-L and collected staff perceptions.</p><p><strong>Design, setting, and participants: </strong>A retrospective, observational, multicenter study with data collected immediately after the patient's death, according to predefined criteria. The study was conducted in 12 ICUs in France. Consecutive patients who died within 48 hours of ICU admission during the study period, in 2022-2023, were included. LST-L decisions were not guided by protocols but were at the discretion of the attending intensivists.</p><p><strong>Main outcomes and measures: </strong>Of 1615 patients admitted to the participating ICUs during the study period, 100 died (6.2%) within 48 hours, including 62 with LST-L.</p><p><strong>Results: </strong>In the LST-L group, age was significantly older (72 yr [64-77.8 yr] vs. 63 yr [59.0-69.8 yr]; p = 0.002), Charlson Comorbidity Index significantly higher (5.5 [2.0-8.0] vs. 4.0 [2.0-5.0]; p < 0.001), and management less invasive compared with the full-care group. By multivariable analysis, male patients were less likely to have LST-L decisions (odds ratio, 0.35; 95% CI, 0.13-0.93; p = 0.03). Most physicians, but a smaller proportion of nurses, perceived LST-L decisions as consensual. For 28 of 100 patients, the intensivist retrospectively deemed the ICU admission not the most suitable option. Patient wishes were rarely considered when making LST-L decisions. Time-limited trials were rarely used. Two-thirds of LST-L decisions were made during on-call hours.</p><p><strong>Conclusions and relevance: </strong>Deaths occurring shortly after ICU admission were usually preceded by LST-L decisions. Efforts are needed to better consider patients' wishes and to strengthen communication between ICU physicians and nursing staff, to ensure appropriate care-even when patients' wishes are unknown and alternatives to ICU admission are not straightforward. Such rare and sometimes unforeseeable cases may also reflect unspoken preferences of patients or their families.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 8","pages":"e1300"},"PeriodicalIF":2.7000,"publicationDate":"2025-08-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12330360/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001300","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: The occurrence of death shortly after ICU admission raises concerns about the appropriateness of providing intensive care to frail patients-many of whom are subsequently subject to decisions to limit life-supporting treatment limitation (LST-L). The proportion of patients who die early and are affected by such limitations remains unknown.
Objectives: The primary objective was to determine the proportion of patients with a decision of LST-L among patients who died within 48 hours after ICU admission. We also conducted analyses to identify variables associated with LST-L and collected staff perceptions.
Design, setting, and participants: A retrospective, observational, multicenter study with data collected immediately after the patient's death, according to predefined criteria. The study was conducted in 12 ICUs in France. Consecutive patients who died within 48 hours of ICU admission during the study period, in 2022-2023, were included. LST-L decisions were not guided by protocols but were at the discretion of the attending intensivists.
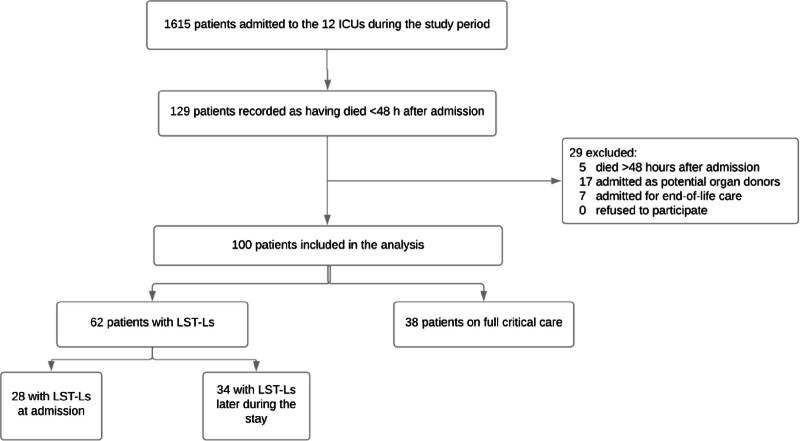
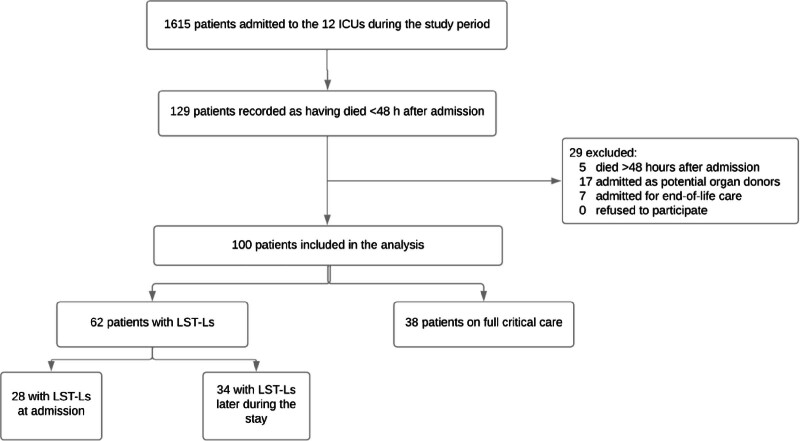
Main outcomes and measures: Of 1615 patients admitted to the participating ICUs during the study period, 100 died (6.2%) within 48 hours, including 62 with LST-L.
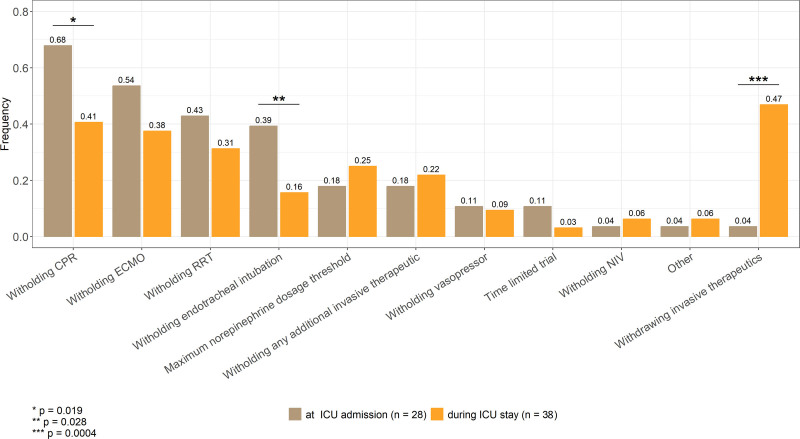
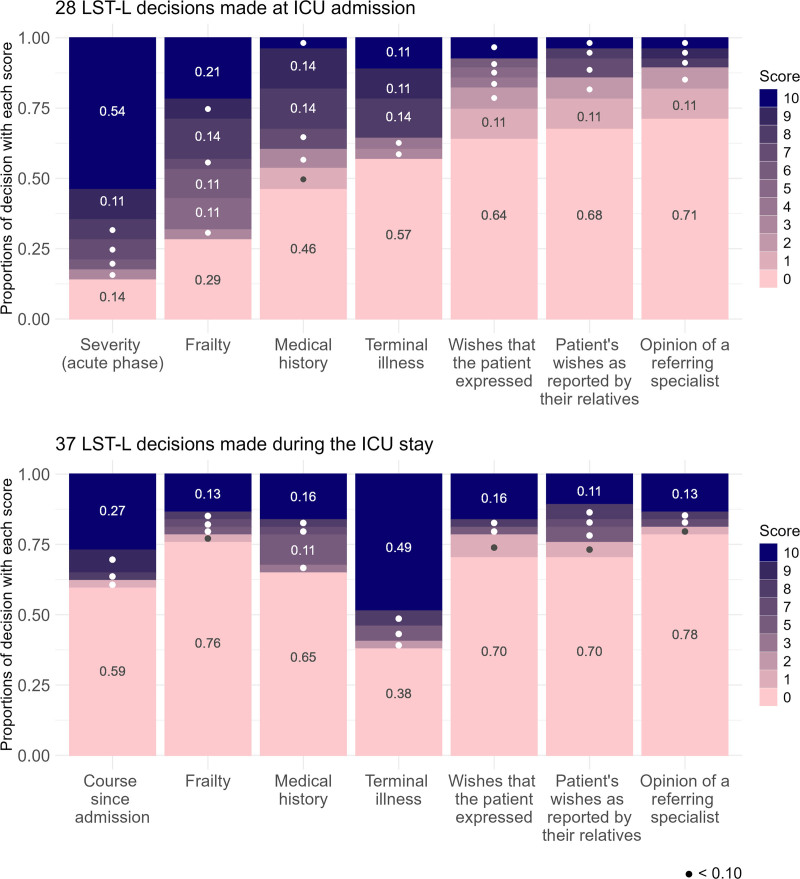
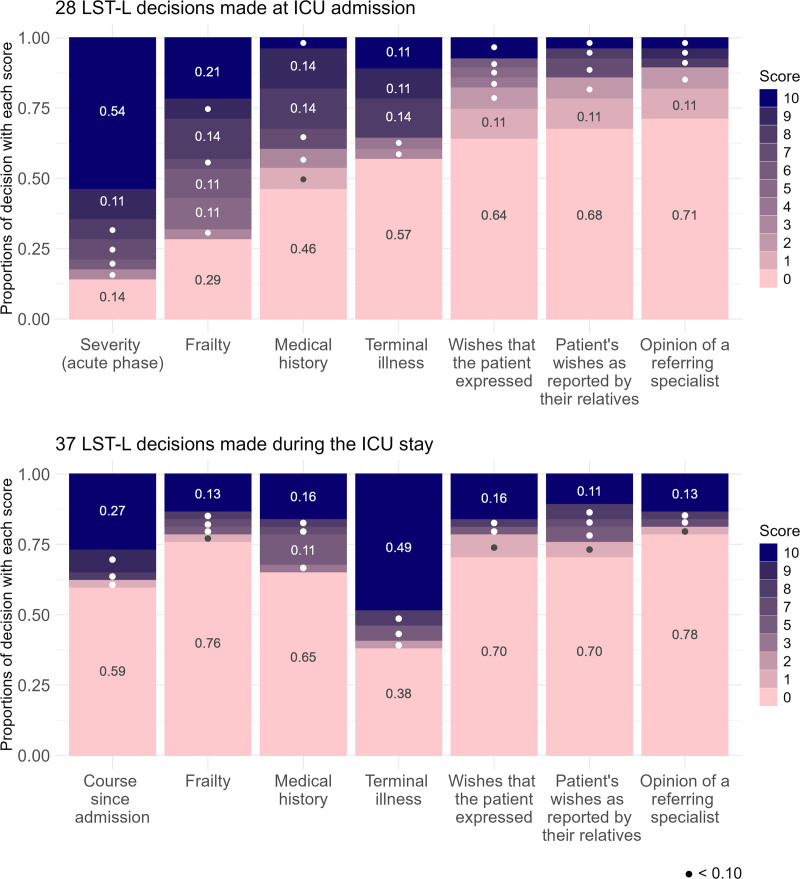
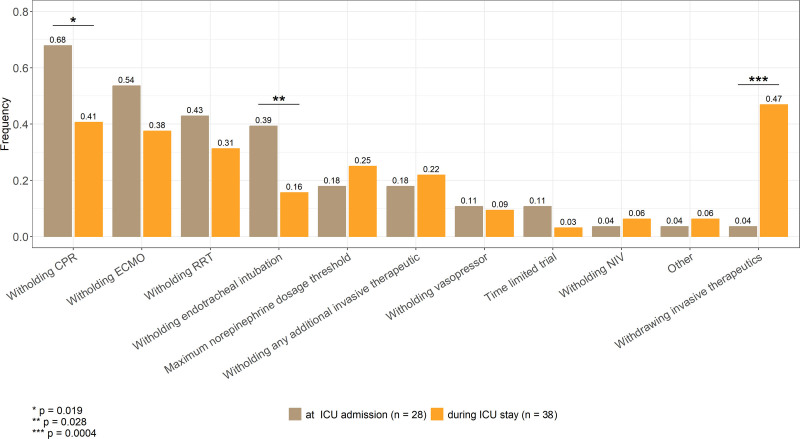
Results: In the LST-L group, age was significantly older (72 yr [64-77.8 yr] vs. 63 yr [59.0-69.8 yr]; p = 0.002), Charlson Comorbidity Index significantly higher (5.5 [2.0-8.0] vs. 4.0 [2.0-5.0]; p < 0.001), and management less invasive compared with the full-care group. By multivariable analysis, male patients were less likely to have LST-L decisions (odds ratio, 0.35; 95% CI, 0.13-0.93; p = 0.03). Most physicians, but a smaller proportion of nurses, perceived LST-L decisions as consensual. For 28 of 100 patients, the intensivist retrospectively deemed the ICU admission not the most suitable option. Patient wishes were rarely considered when making LST-L decisions. Time-limited trials were rarely used. Two-thirds of LST-L decisions were made during on-call hours.
Conclusions and relevance: Deaths occurring shortly after ICU admission were usually preceded by LST-L decisions. Efforts are needed to better consider patients' wishes and to strengthen communication between ICU physicians and nursing staff, to ensure appropriate care-even when patients' wishes are unknown and alternatives to ICU admission are not straightforward. Such rare and sometimes unforeseeable cases may also reflect unspoken preferences of patients or their families.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


