Durval Renato Wohnrath, Raphael de Oliveira E Silva, Raphael Leonardo Cunha Araujo
{"title":"Siewert II esophagogastric junction cancer: total gastrectomy or esophagectomy?","authors":"Durval Renato Wohnrath, Raphael de Oliveira E Silva, Raphael Leonardo Cunha Araujo","doi":"10.1590/0102-67202025000019e1888","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The surgical approach for esophagogastric junction cancers (EJC), Siewert II, has been controversial regarding margin control, reconstruction, and lymphadenectomy extension. Therefore, predicting the need for total/subtotal esophagectomy and proximal gastrectomy (TEPG) or total gastrectomy with distal esophagectomy (TGDE) can be challenging, with each direction usually excluding the other. Historically, complication rates for TEPG are higher, affecting further systemic treatment and long-term outcomes.</p><p><strong>Aims: </strong>The aim of this study was to describe a surgical strategy for approaching tumors such as Siewert II EGJ, with the intraoperative decision to perform total gastrectomy with lymphadenectomy D2 or esophagectomy with lymphadenectomy based on intraoperative frozen sections.</p><p><strong>Methods: </strong>All patients underwent laparotomy, beginning with greater curvature detachment while preserving the right gastroepiploic, right and left gastric arteries; dissection of the esophageal hiatus for node harvesting; and transection of the distal esophagus and its frozen section. TGDE was preferred if the proximal margin of the distal esophagus was negative; TEPG and gastric tube reconstruction were performed through transhiatal access if the margin was positive.</p><p><strong>Results: </strong>Among 38 Siewert II patients, 26 (69%) underwent TGDE and 12 (31%) underwent TEPG, regardless of the trend toward higher complication rates, positive margins, and shorter overall survival in the TEPG group, no statistically significant differences were detected.</p><p><strong>Conclusions: </strong>Although no significant differences in morbidity between the two procedures were noted, type II errors could be a possible cause. This study suggests that unnecessary esophagectomies can be avoided without jeopardizing surgical or oncologic outcomes by opting for a less morbid procedure.</p>","PeriodicalId":72298,"journal":{"name":"Arquivos brasileiros de cirurgia digestiva : ABCD = Brazilian archives of digestive surgery","volume":"38 ","pages":"e1888"},"PeriodicalIF":1.8000,"publicationDate":"2025-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12324771/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arquivos brasileiros de cirurgia digestiva : ABCD = Brazilian archives of digestive surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1590/0102-67202025000019e1888","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The surgical approach for esophagogastric junction cancers (EJC), Siewert II, has been controversial regarding margin control, reconstruction, and lymphadenectomy extension. Therefore, predicting the need for total/subtotal esophagectomy and proximal gastrectomy (TEPG) or total gastrectomy with distal esophagectomy (TGDE) can be challenging, with each direction usually excluding the other. Historically, complication rates for TEPG are higher, affecting further systemic treatment and long-term outcomes.
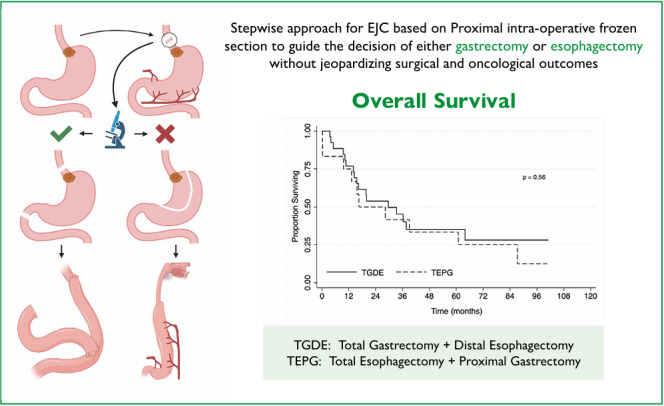
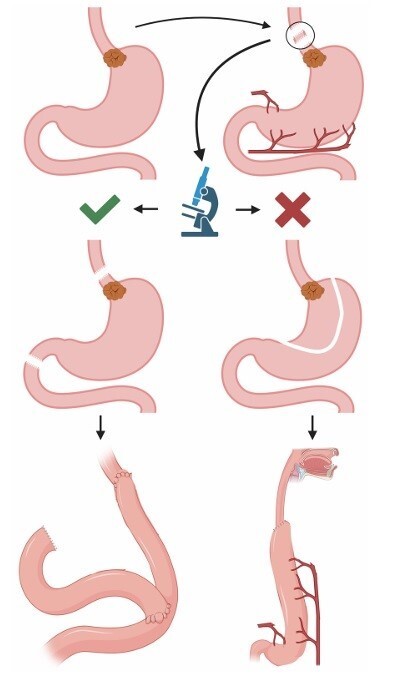
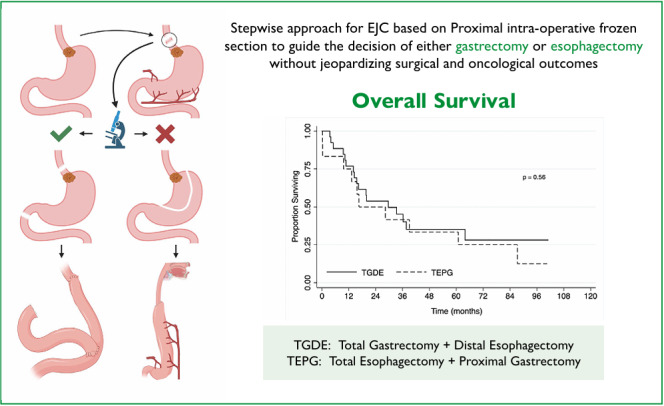
Aims: The aim of this study was to describe a surgical strategy for approaching tumors such as Siewert II EGJ, with the intraoperative decision to perform total gastrectomy with lymphadenectomy D2 or esophagectomy with lymphadenectomy based on intraoperative frozen sections.
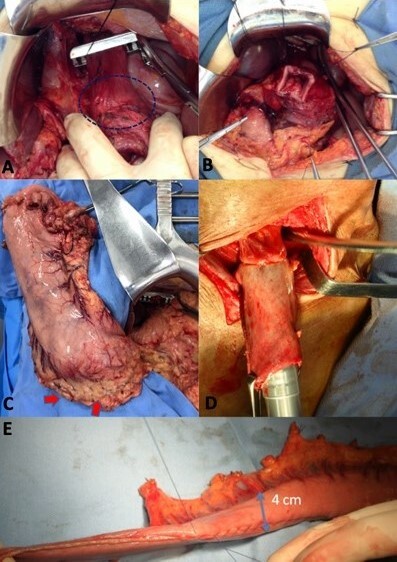
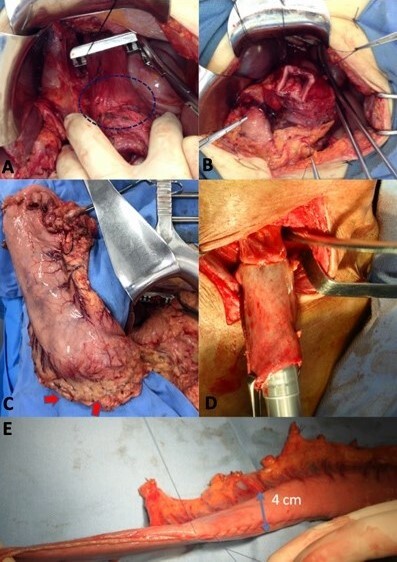
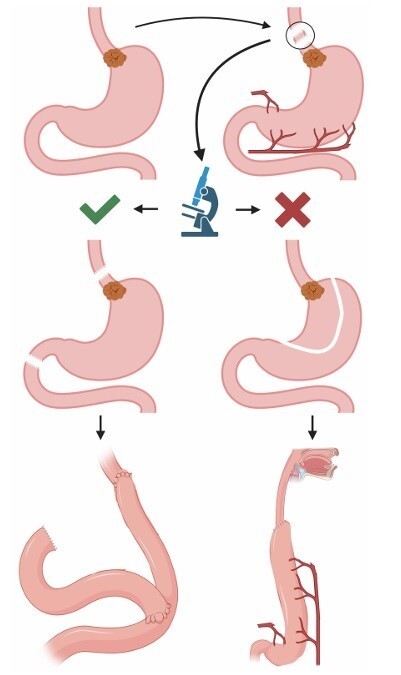
Methods: All patients underwent laparotomy, beginning with greater curvature detachment while preserving the right gastroepiploic, right and left gastric arteries; dissection of the esophageal hiatus for node harvesting; and transection of the distal esophagus and its frozen section. TGDE was preferred if the proximal margin of the distal esophagus was negative; TEPG and gastric tube reconstruction were performed through transhiatal access if the margin was positive.
Results: Among 38 Siewert II patients, 26 (69%) underwent TGDE and 12 (31%) underwent TEPG, regardless of the trend toward higher complication rates, positive margins, and shorter overall survival in the TEPG group, no statistically significant differences were detected.
Conclusions: Although no significant differences in morbidity between the two procedures were noted, type II errors could be a possible cause. This study suggests that unnecessary esophagectomies can be avoided without jeopardizing surgical or oncologic outcomes by opting for a less morbid procedure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


