Ioana B Florea, Nadia H Bakir, Meghan O Kelly, Joel D Schilling, Gregory A Ewald, Akinobu Itoh, Marc R Moon, Spencer J Melby, Ralph J Damiano, Kunal D Kotkar, Muhammad F Masood
{"title":"Risk Factors for Development of Stroke in Patients With Continuous-Flow Left Ventricular Assist Device Support as Destination Therapy.","authors":"Ioana B Florea, Nadia H Bakir, Meghan O Kelly, Joel D Schilling, Gregory A Ewald, Akinobu Itoh, Marc R Moon, Spencer J Melby, Ralph J Damiano, Kunal D Kotkar, Muhammad F Masood","doi":"10.14503/THIJ-23-8332","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Continuous-flow left ventricular assist devices (LVADs) are increasingly used as destination therapy. Although postimplantation stroke rates have been described in the context of bridge-to-transplant or mixed cohorts, stroke development is not well evaluated in patients who receive continuous-flow LVAD with a destination therapy indication. This report characterizes the stroke profile of a modern institutional cohort of patients undergoing destination therapy and evaluates their risk factors for stroke onset.</p><p><strong>Methods: </strong>Patients implanted with continuous-flow LVAD as destination therapy at the reporting institution between January 2010 and June 2020 were retrospectively reviewed and analyzed. Stroke was defined as any neurologic deficit caused by an abrupt disruption in cerebral blood flow that did not resolve within 24 hours and that was confirmed by imaging. Terminal outcomes of stroke development and death were assessed using a competing-risks model. Fine-Gray regression was used to evaluate potential predictors of stroke development.</p><p><strong>Results: </strong>Patients who received continuous-flow LVAD (N = 311) were classified by device type: Heart-Mate II (Abbott; n = 97); HeartMate 3 (Abbott; n = 72); and HeartWare Ventricular Assist Device (Medtronic; n = 42). Thirty-five percent of patients (110/311) developed postoperative atrial fibrillation (AF). Estimated stroke incidence was 15% at 1 year, 24% at 3 years, and 27% at 5 years. According to multivariable Fine-Gray regression, receiving a HeartMate 3 device (subdistribution hazard ratio [HR], 0.41 [95% CI, 0.19-0.90]; <i>P</i> = .03) and amiodarone at discharge (HR, 0.55 [95% CI, 0.33-0.94]; <i>P</i> = .03) were associated with lower stroke risk. Postoperative AF (HR, 1.68 [95% CI, 1.03-2.73]; <i>P</i> = .04) was associated with increased stroke risk.</p><p><strong>Conclusion: </strong>The HeartMate 3 was associated with decreased stroke rates, but risk remained high for patients who developed postoperative AF. Further investigation into protective strategies and use of amiodarone to treat AF after continuous-flow LVAD implantation is needed.</p>","PeriodicalId":48680,"journal":{"name":"Texas Heart Institute Journal","volume":"52 2","pages":"e238332"},"PeriodicalIF":0.9000,"publicationDate":"2025-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12322576/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Texas Heart Institute Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14503/THIJ-23-8332","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Continuous-flow left ventricular assist devices (LVADs) are increasingly used as destination therapy. Although postimplantation stroke rates have been described in the context of bridge-to-transplant or mixed cohorts, stroke development is not well evaluated in patients who receive continuous-flow LVAD with a destination therapy indication. This report characterizes the stroke profile of a modern institutional cohort of patients undergoing destination therapy and evaluates their risk factors for stroke onset.
Methods: Patients implanted with continuous-flow LVAD as destination therapy at the reporting institution between January 2010 and June 2020 were retrospectively reviewed and analyzed. Stroke was defined as any neurologic deficit caused by an abrupt disruption in cerebral blood flow that did not resolve within 24 hours and that was confirmed by imaging. Terminal outcomes of stroke development and death were assessed using a competing-risks model. Fine-Gray regression was used to evaluate potential predictors of stroke development.
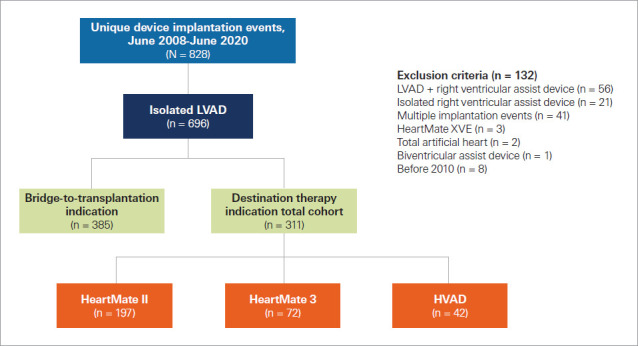
Results: Patients who received continuous-flow LVAD (N = 311) were classified by device type: Heart-Mate II (Abbott; n = 97); HeartMate 3 (Abbott; n = 72); and HeartWare Ventricular Assist Device (Medtronic; n = 42). Thirty-five percent of patients (110/311) developed postoperative atrial fibrillation (AF). Estimated stroke incidence was 15% at 1 year, 24% at 3 years, and 27% at 5 years. According to multivariable Fine-Gray regression, receiving a HeartMate 3 device (subdistribution hazard ratio [HR], 0.41 [95% CI, 0.19-0.90]; P = .03) and amiodarone at discharge (HR, 0.55 [95% CI, 0.33-0.94]; P = .03) were associated with lower stroke risk. Postoperative AF (HR, 1.68 [95% CI, 1.03-2.73]; P = .04) was associated with increased stroke risk.
Conclusion: The HeartMate 3 was associated with decreased stroke rates, but risk remained high for patients who developed postoperative AF. Further investigation into protective strategies and use of amiodarone to treat AF after continuous-flow LVAD implantation is needed.
期刊介绍:
For more than 45 years, the Texas Heart Institute Journal has been published by the Texas Heart Institute as part of its medical education program. Our bimonthly peer-reviewed journal enjoys a global audience of physicians, scientists, and healthcare professionals who are contributing to the prevention, diagnosis, and treatment of cardiovascular disease.
The Journal was printed under the name of Cardiovascular Diseases from 1974 through 1981 (ISSN 0093-3546). The name was changed to Texas Heart Institute Journal in 1982 and was printed through 2013 (ISSN 0730-2347). In 2014, the Journal moved to online-only publication. It is indexed by Index Medicus/MEDLINE and by other indexing and abstracting services worldwide. Our full archive is available at PubMed Central.
The Journal invites authors to submit these article types for review:
-Clinical Investigations-
Laboratory Investigations-
Reviews-
Techniques-
Coronary Anomalies-
History of Medicine-
Case Reports/Case Series (Submission Fee: $70.00 USD)-
Images in Cardiovascular Medicine (Submission Fee: $35.00 USD)-
Guest Editorials-
Peabody’s Corner-
Letters to the Editor

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


