{"title":"Multimorbidity progression and the heterogeneous impact of healthy ageing risk factors: a multicohort study.","authors":"Shasha Han, Wangyue Chen, Muzi Shen, Ruitai Shao, Weizhong Yang, Chen Wang","doi":"10.1136/bmjph-2024-002474","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>We aimed to quantify how diseases accumulate and diminish among ageing populations, and examine how modifiable risk factors influence these progressions.</p><p><strong>Methods: </strong>In this multicohort study with four cohorts, China Health and Retirement Longitudinal Study, the English Longitudinal Study of Ageing (ELSA), the Health and Retirement Study, and the Survey of Health, Ageing and Retirement in Europe (SHARE), and 75 874 participants, we employed a multistage model that accommodated bidirectional transitions between four health stages (0, 1, 2, ≥3 conditions) from baseline to 8 years, and conducted matching analyses to examine the influence of age, sex, socioeconomic status (SES) and lifestyle factors on these transitions.</p><p><strong>Results: </strong>Disease accumulated faster than diminished (0.08-0.44 vs 0.00-0.06). Transitions accelerated towards severe multimorbidity (0→1: 0.29 (95% CI 0.28 to 0.29), 1→2: 0.27 (95% CI 0.27 to 0.28) and 2→≥3: 0.44 (95% CI 0.43 to 0.45)). Mortality risk escalated with condition count: 0.08 (95% CI 0.08 to 0.09) for 0 conditions, 0.13 (95% CI 0.12 to 0.13) for 1 condition 0.17 (95% CI 0.16 to 0.18) for 2 conditions, and 0.27 (95% CI 0.26 to 0.27) for ≥3 conditions. Cohorts exhibited broadly similar progression patterns, though ELSA demonstrated slower transitions to ≥3 conditions and SHARE showed elevated mortality from 0 and 1 conditions. Key risk factor effects emerged: disease accumulation peaked at 55-65 years; females had higher disease accumulation but lower transitions to death than males; Low-SES populations had higher probabilities of developing ≥3 conditions than the middle-SES group, while middle-SES populations had higher accumulation probabilities for 0→≥2 and 2→≥3. Lifestyle factors exerted differential impacts: smoking increased 1→3 transitions and drinking increased 0→2 transitions, while physician inactivity increased 0→3 transitions. Sensitivity analyses confirmed robustness across 11 condition-specific models.</p><p><strong>Conclusions: </strong>Multimorbidity progression accelerates nonlinearly, with risk factors exerting varying effects, depending on the magnitude of risk factors and initial health states. Precision interventions should target age, sex, SES and lifestyle-specific strategies.</p>","PeriodicalId":101362,"journal":{"name":"BMJ public health","volume":"3 2","pages":"e002474"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12320038/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ public health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjph-2024-002474","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: We aimed to quantify how diseases accumulate and diminish among ageing populations, and examine how modifiable risk factors influence these progressions.
Methods: In this multicohort study with four cohorts, China Health and Retirement Longitudinal Study, the English Longitudinal Study of Ageing (ELSA), the Health and Retirement Study, and the Survey of Health, Ageing and Retirement in Europe (SHARE), and 75 874 participants, we employed a multistage model that accommodated bidirectional transitions between four health stages (0, 1, 2, ≥3 conditions) from baseline to 8 years, and conducted matching analyses to examine the influence of age, sex, socioeconomic status (SES) and lifestyle factors on these transitions.
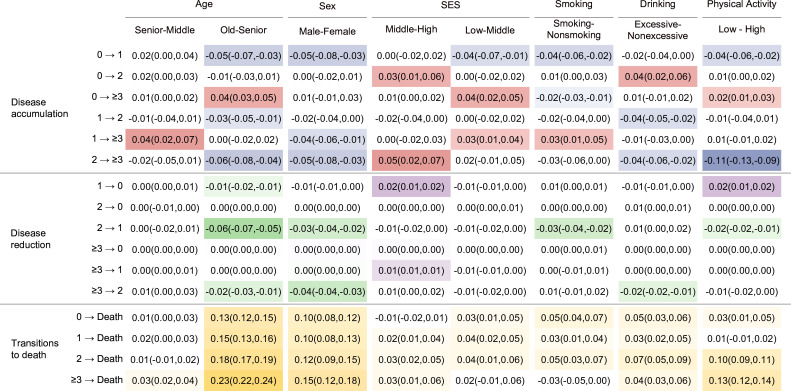
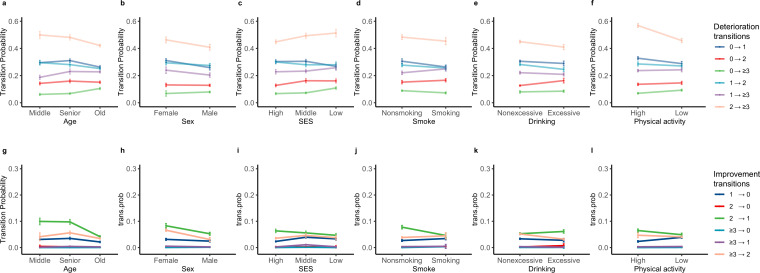
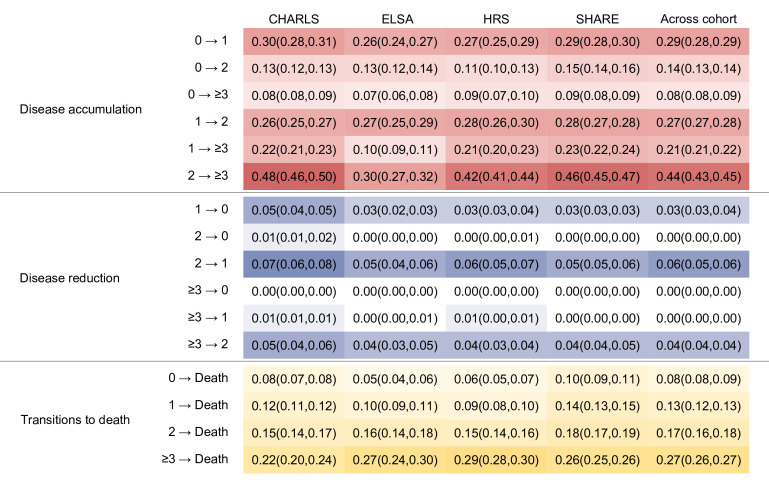
Results: Disease accumulated faster than diminished (0.08-0.44 vs 0.00-0.06). Transitions accelerated towards severe multimorbidity (0→1: 0.29 (95% CI 0.28 to 0.29), 1→2: 0.27 (95% CI 0.27 to 0.28) and 2→≥3: 0.44 (95% CI 0.43 to 0.45)). Mortality risk escalated with condition count: 0.08 (95% CI 0.08 to 0.09) for 0 conditions, 0.13 (95% CI 0.12 to 0.13) for 1 condition 0.17 (95% CI 0.16 to 0.18) for 2 conditions, and 0.27 (95% CI 0.26 to 0.27) for ≥3 conditions. Cohorts exhibited broadly similar progression patterns, though ELSA demonstrated slower transitions to ≥3 conditions and SHARE showed elevated mortality from 0 and 1 conditions. Key risk factor effects emerged: disease accumulation peaked at 55-65 years; females had higher disease accumulation but lower transitions to death than males; Low-SES populations had higher probabilities of developing ≥3 conditions than the middle-SES group, while middle-SES populations had higher accumulation probabilities for 0→≥2 and 2→≥3. Lifestyle factors exerted differential impacts: smoking increased 1→3 transitions and drinking increased 0→2 transitions, while physician inactivity increased 0→3 transitions. Sensitivity analyses confirmed robustness across 11 condition-specific models.
Conclusions: Multimorbidity progression accelerates nonlinearly, with risk factors exerting varying effects, depending on the magnitude of risk factors and initial health states. Precision interventions should target age, sex, SES and lifestyle-specific strategies.
前言:我们的目的是量化疾病如何在老龄化人群中积累和减少,并检查可改变的风险因素如何影响这些进展。方法:在这项包括中国健康与退休纵向研究、英国老龄化纵向研究(ELSA)、健康与退休研究和欧洲健康、老龄化和退休调查(SHARE)四个队列和75 874名参与者的多队列研究中,我们采用了一个多阶段模型,该模型适应了从基线到8岁四个健康阶段(0、1、2、≥3个条件)之间的双向过渡,并进行了匹配分析,以检验年龄、性别、社会经济地位(SES)和生活方式因素对这些转变的影响。结果:病变累积快于消退(0.08 ~ 0.44 vs 0.000 ~ 0.06)。过渡加速到严重的多重疾病(0→1:0.29 (95% CI 0.28至0.29),1→2:0.27 (95% CI 0.27至0.28)和2→≥3:0.44 (95% CI 0.43至0.45))。死亡风险随着病情数的增加而增加:0种情况为0.08 (95% CI 0.08 ~ 0.09), 1种情况为0.13 (95% CI 0.12 ~ 0.13), 2种情况为0.17 (95% CI 0.16 ~ 0.18),≥3种情况为0.27 (95% CI 0.26 ~ 0.27)。队列表现出大致相似的进展模式,尽管ELSA表现出向≥3种情况的缓慢过渡,SHARE显示从0和1种情况的死亡率升高。出现了关键的风险因素影响:疾病积累在55-65岁达到高峰;女性的疾病积累高于男性,但死亡过渡低于男性;低ses群体出现≥3个条件的概率高于中等ses群体,而中等ses群体0→≥2和2→≥3的积累概率较高。生活方式因素有不同程度的影响,吸烟增加1→3个转变,饮酒增加0→2个转变,不运动增加0→3个转变。敏感性分析证实了11个特定条件模型的稳健性。结论:多病进展呈非线性加速,危险因素发挥不同的作用,取决于危险因素的大小和初始健康状态。精准干预应针对特定年龄、性别、社会经济地位和生活方式的策略。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


