Jie Chen, Hui Cheng, Yi-Fu Li, Yu-Chen Li, Hao-Xiang Long, Jie-Yi Lin, Chun Fung Tse, Bo-Wen Shen, Pan Wang, Sai-Lan Liu, Shan-Shan Guo, Shu-Ming Liang, Qiu-Yan Chen, Lin-Quan Tang, Hai-Qiang Mai, Li-Ting Liu
{"title":"Real-world experience on efficacy and safety of different adjuvant chemotherapy regimens in locoregionally advanced nasopharyngeal carcinoma.","authors":"Jie Chen, Hui Cheng, Yi-Fu Li, Yu-Chen Li, Hao-Xiang Long, Jie-Yi Lin, Chun Fung Tse, Bo-Wen Shen, Pan Wang, Sai-Lan Liu, Shan-Shan Guo, Shu-Ming Liang, Qiu-Yan Chen, Lin-Quan Tang, Hai-Qiang Mai, Li-Ting Liu","doi":"10.1136/bmjonc-2024-000718","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study aimed to evaluate the efficacy and toxicity of various adjuvant chemotherapy (AC) regimens for treating locoregionally advanced nasopharyngeal carcinoma.</p><p><strong>Methods and analysis: </strong>In this retrospective study, the patients received either intravenous AC regimens (cisplatin-fluorouracil (PF) or cisplatin-gemcitabine (GP)) or oral regimens (capecitabine or tegafur, gimeracil and oteracil potassium capsule (S-1)) following concurrent chemoradiotherapy (CCRT). The primary endpoint was progression-free survival (PFS).</p><p><strong>Results: </strong>A total of 229 patients were documented in the oral administration group (127 patients received capecitabine and 102 received S-1), whereas 241 patients were recorded in the intravenous group (164 patients received the PF regimen and 77 received the GP regimen). There was no significant difference in PFS between the intravenous and oral groups (n=154 each) after propensity score matching (3-year PFS rate: 76.3% vs 73.9%; HR, 0.803; 95% CI 0.523 to 1.233, p=0.316). However, based on the overall cohort, the GP regimen showed a superior 3-year PFS rate (89.1%) compared with PF (74.6%), capecitabine (76.0%) and S-1 (74.3%) regimen (p=0.005, 0.012 and 0.003, respectively), while multivariable analyses also demonstrated that the GP regimen (HR<sub>PFS</sub>, 0.38; 95% CI 0.18 to 0.81, p=0.012) was associated with better survival. Additionally, the intravenous group, which included PF and GP, exhibited a higher incidence of grade≥3 leucocytopenia (50.0% vs 22.7%), neutropenia (30.5% vs 18.2%), anaemia (16.2% vs 3.9%), hyponatraemia (3.2% vs 0) and hypokalaemia (12.3% vs 4.5%) than the oral group.</p><p><strong>Conclusion: </strong>For patients treated with upfront CCRT, AC should be considered, and intravenous GP is preferred, although patients should be counselled about an increased risk of haematological toxicities. For patients treated with induction chemotherapy and CCRT, oral chemotherapy, either with capecitabine or S-1, was efficacious and tolerable.</p>","PeriodicalId":72436,"journal":{"name":"BMJ oncology","volume":"4 1","pages":"e000718"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12320049/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjonc-2024-000718","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: This study aimed to evaluate the efficacy and toxicity of various adjuvant chemotherapy (AC) regimens for treating locoregionally advanced nasopharyngeal carcinoma.
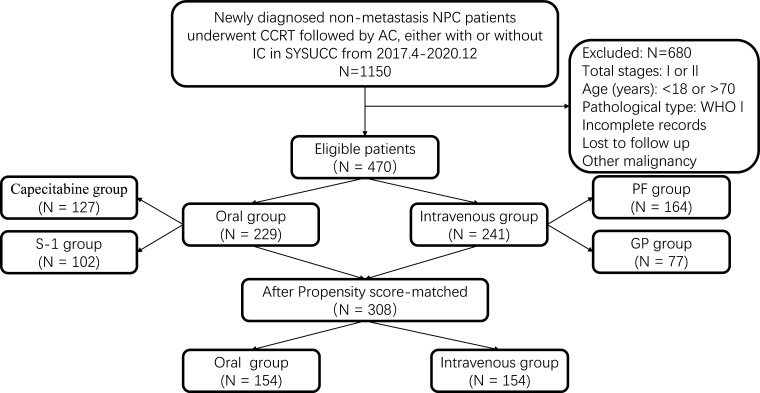
Methods and analysis: In this retrospective study, the patients received either intravenous AC regimens (cisplatin-fluorouracil (PF) or cisplatin-gemcitabine (GP)) or oral regimens (capecitabine or tegafur, gimeracil and oteracil potassium capsule (S-1)) following concurrent chemoradiotherapy (CCRT). The primary endpoint was progression-free survival (PFS).
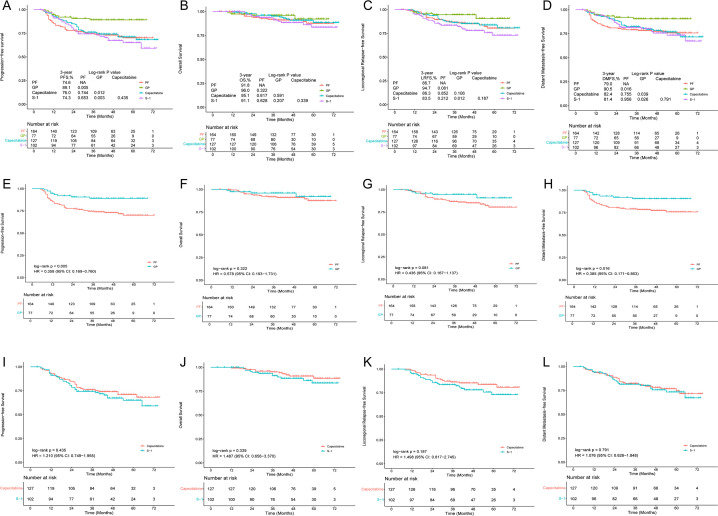
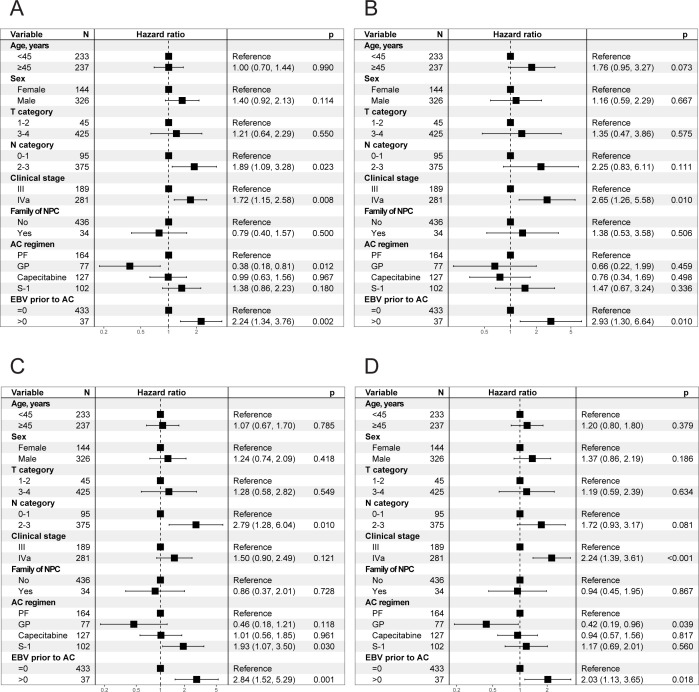
Results: A total of 229 patients were documented in the oral administration group (127 patients received capecitabine and 102 received S-1), whereas 241 patients were recorded in the intravenous group (164 patients received the PF regimen and 77 received the GP regimen). There was no significant difference in PFS between the intravenous and oral groups (n=154 each) after propensity score matching (3-year PFS rate: 76.3% vs 73.9%; HR, 0.803; 95% CI 0.523 to 1.233, p=0.316). However, based on the overall cohort, the GP regimen showed a superior 3-year PFS rate (89.1%) compared with PF (74.6%), capecitabine (76.0%) and S-1 (74.3%) regimen (p=0.005, 0.012 and 0.003, respectively), while multivariable analyses also demonstrated that the GP regimen (HRPFS, 0.38; 95% CI 0.18 to 0.81, p=0.012) was associated with better survival. Additionally, the intravenous group, which included PF and GP, exhibited a higher incidence of grade≥3 leucocytopenia (50.0% vs 22.7%), neutropenia (30.5% vs 18.2%), anaemia (16.2% vs 3.9%), hyponatraemia (3.2% vs 0) and hypokalaemia (12.3% vs 4.5%) than the oral group.
Conclusion: For patients treated with upfront CCRT, AC should be considered, and intravenous GP is preferred, although patients should be counselled about an increased risk of haematological toxicities. For patients treated with induction chemotherapy and CCRT, oral chemotherapy, either with capecitabine or S-1, was efficacious and tolerable.
目的:评价不同辅助化疗方案治疗局部进展期鼻咽癌的疗效和毒副作用。方法和分析:在这项回顾性研究中,患者在同步放化疗(CCRT)后接受静脉交流方案(顺铂-氟尿嘧啶(PF)或顺铂-吉西他滨(GP))或口服方案(卡培他滨或替加富、吉美拉西和奥他嘧啶钾胶囊(S-1))。主要终点为无进展生存期(PFS)。结果:口服组229例(卡培他滨127例,S-1 102例),静脉注射组241例(PF方案164例,GP方案77例)。倾向评分匹配后,静脉注射组和口服组(n=154)的PFS无显著差异(3年PFS率:76.3% vs 73.9%;人力资源,0.803;95% CI 0.523 ~ 1.233, p=0.316)。然而,基于整体队列,GP方案的3年PFS率(89.1%)优于PF(74.6%)、卡培他滨(76.0%)和S-1(74.3%)方案(p分别=0.005、0.012和0.003),而多变量分析也表明GP方案(HRPFS, 0.38;95% CI 0.18 ~ 0.81, p=0.012)与较好的生存率相关。此外,静脉注射组(包括PF和GP)出现≥3级白细胞减少症(50.0% vs 22.7%)、中性粒细胞减少症(30.5% vs 18.2%)、贫血(16.2% vs 3.9%)、低钠血症(3.2% vs 0)和低钾血症(12.3% vs 4.5%)的发生率高于口服组。结论:对于接受前期CCRT治疗的患者,应考虑AC,首选静脉GP,但应告知患者血液学毒性风险增加。对于接受诱导化疗和CCRT的患者,口服化疗,无论是卡培他滨还是S-1,都是有效且耐受的。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


