Microbial profiling of community-acquired pneumonia in patients with and without chronic obstructive pulmonary disease: a comprehensive molecular diagnostics study.
Dagfinn Lunde Markussen, Christoffer Lindemann, Sondre Serigstad, Synne Jenum, Christian Ritz, Harleen M S Grewal
{"title":"Microbial profiling of community-acquired pneumonia in patients with and without chronic obstructive pulmonary disease: a comprehensive molecular diagnostics study.","authors":"Dagfinn Lunde Markussen, Christoffer Lindemann, Sondre Serigstad, Synne Jenum, Christian Ritz, Harleen M S Grewal","doi":"10.1186/s41479-025-00172-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Community-acquired pneumonia (CAP) causes substantial morbidity and mortality, particularly in patients with chronic obstructive pulmonary disease (COPD). This study compares the microbial detections in CAP patients with and without COPD using culture based and molecular diagnostic methods.</p><p><strong>Methods: </strong>This prospective study included 412 hospitalized pneumonia patients (136 with COPD). Lower respiratory tract samples were analysed with traditional cultures and a multiplex PCR panel (FilmArray Pneumonia Panel Plus). Multivariable Poisson regression identified predictors of Pseudomonas aeruginosa detection, and logistic regression estimated detection probability using the top predictors.</p><p><strong>Results: </strong>Overall pathogen detection rates were similar between groups, but P. aeruginosa was significantly more common in COPD patients (12.5% vs. 3.1%; p < 0.001). In adjusted analyses, each additional year of age increased the risk of P. aeruginosa by 5% (RR 1.05; 95% CI 1.01-1.09), while advanced COPD (GOLD 3-4) conferred a four-fold higher risk (RR 4.29; 95% CI 1.94-9.46), diabetes mellitus a four-fold risk (RR 4.04; 95% CI 1.97-8.29), and prior P. aeruginosa detection a five-fold risk (RR 5.03; 95% CI 2.44-10.36). Inhaler use, bronchiectasis, and recent hospitalization were not independently associated.</p><p><strong>Conclusion: </strong>Although overall microbial detection rates were comparable between groups, P. aeruginosa was disproportionately prevalent in high-risk COPD individuals. While most COPD patients with pneumonia can be managed with standard empirical antibiotics, empirical coverage for P. aeruginosa should be considered for selected high-risk patients. Prospective studies are warranted to evaluate targeted P. aeruginosa coverage to optimize antibiotic stewardship and improve outcomes.</p>","PeriodicalId":45120,"journal":{"name":"Pneumonia","volume":"17 1","pages":"19"},"PeriodicalIF":6.2000,"publicationDate":"2025-08-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12323216/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pneumonia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41479-025-00172-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Community-acquired pneumonia (CAP) causes substantial morbidity and mortality, particularly in patients with chronic obstructive pulmonary disease (COPD). This study compares the microbial detections in CAP patients with and without COPD using culture based and molecular diagnostic methods.
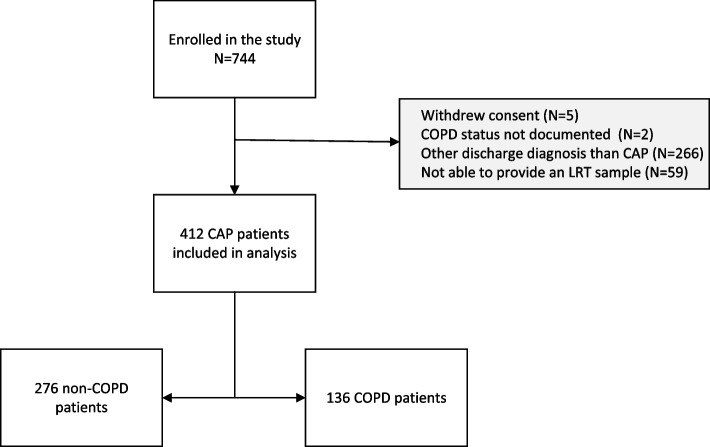
Methods: This prospective study included 412 hospitalized pneumonia patients (136 with COPD). Lower respiratory tract samples were analysed with traditional cultures and a multiplex PCR panel (FilmArray Pneumonia Panel Plus). Multivariable Poisson regression identified predictors of Pseudomonas aeruginosa detection, and logistic regression estimated detection probability using the top predictors.
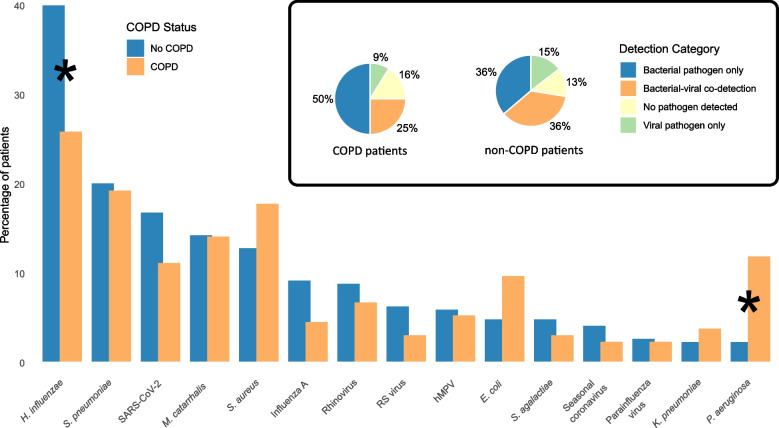
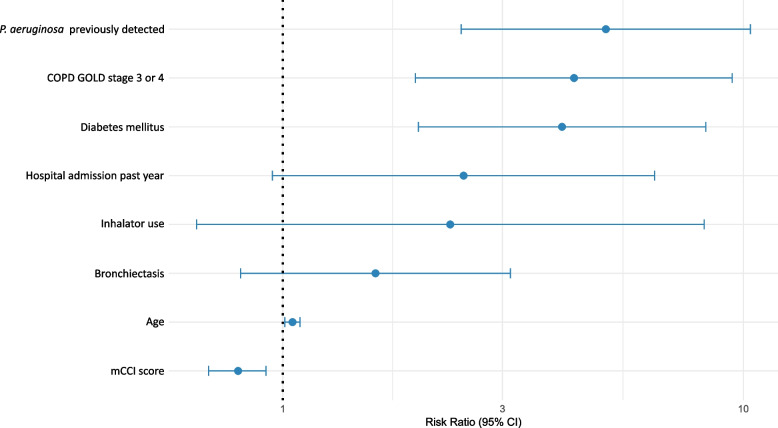
Results: Overall pathogen detection rates were similar between groups, but P. aeruginosa was significantly more common in COPD patients (12.5% vs. 3.1%; p < 0.001). In adjusted analyses, each additional year of age increased the risk of P. aeruginosa by 5% (RR 1.05; 95% CI 1.01-1.09), while advanced COPD (GOLD 3-4) conferred a four-fold higher risk (RR 4.29; 95% CI 1.94-9.46), diabetes mellitus a four-fold risk (RR 4.04; 95% CI 1.97-8.29), and prior P. aeruginosa detection a five-fold risk (RR 5.03; 95% CI 2.44-10.36). Inhaler use, bronchiectasis, and recent hospitalization were not independently associated.
Conclusion: Although overall microbial detection rates were comparable between groups, P. aeruginosa was disproportionately prevalent in high-risk COPD individuals. While most COPD patients with pneumonia can be managed with standard empirical antibiotics, empirical coverage for P. aeruginosa should be considered for selected high-risk patients. Prospective studies are warranted to evaluate targeted P. aeruginosa coverage to optimize antibiotic stewardship and improve outcomes.
背景:社区获得性肺炎(CAP)引起大量发病率和死亡率,特别是慢性阻塞性肺疾病(COPD)患者。本研究比较了基于培养和分子诊断方法在伴有和不伴有COPD的CAP患者中的微生物检测结果。方法:本前瞻性研究纳入412例住院肺炎患者(其中136例合并COPD)。下呼吸道样本采用传统培养和多重PCR检测板(FilmArray肺炎检测板Plus)进行分析。多变量泊松回归确定铜绿假单胞菌检测的预测因子,logistic回归利用最高预测因子估计检测概率。结果:两组间的总体病原体检出率相似,但P. aeruginosa在COPD患者中更为常见(12.5% vs. 3.1%;p结论:尽管两组间的微生物检出率具有可比性,但铜绿假单胞菌在COPD高危人群中尤为普遍。虽然大多数COPD合并肺炎患者可以使用标准经验性抗生素进行治疗,但应考虑对选定的高风险患者进行铜绿假单胞菌的经验性覆盖。有必要进行前瞻性研究,以评估有针对性的铜绿假单胞菌覆盖范围,以优化抗生素管理并改善结果。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


