Mitchell Sarkies, Nicholas Murphy, Ramya Kunnath, Seth Tarrant, Erica Epstein, Natasha Weaver, Cameron R Hemmert, Zsolt J Balogh
{"title":"Avoidable and unavoidable delays in hip fracture surgery : a prospective observational study of who, what, and why?","authors":"Mitchell Sarkies, Nicholas Murphy, Ramya Kunnath, Seth Tarrant, Erica Epstein, Natasha Weaver, Cameron R Hemmert, Zsolt J Balogh","doi":"10.1302/2633-1462.68.BJO-2025-0083.R1","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Surgical management of hip fracture is often delayed, which is associated with increased mortality. We aimed to prospectively determine the proportion of potentially avoidable delay to surgery beyond 48 hours, and its causes, as clinically relevant margins for quality improvement.</p><p><strong>Methods: </strong>A 12-month prospective cohort study from September 2022 to September 2023 was conducted on all 427 hip fracture surgery patients aged ≥ 50 years who were admitted to a trauma centre in New South Wales, Australia. The reasons for delay, medical speciality, and level of seniority initiating the decision, and what response was taken after the delay, were recorded for each case delayed beyond 48 hours from hospital admission. Surgical delays were categorized as either avoidable or unavoidable independently by surgical and medical experts.</p><p><strong>Results: </strong>From 427 hip fractures, 37% (160/427) had surgery beyond 48 hours, with 29% (124/427) considered avoidable, 6% (27/427) unavoidable, and 2% (9/427) unable to be categorized. Patients experienced a median 43-hour time to surgery (IQR 27 to 63): 30 hours (IQR 24 to 41) for non-delayed, 69 hours (IQR 55 to 93) for avoidable, and 75 hours (IQR 59 to 135) for unavoidable delays. Patients with unavoidable delays had higher American Society of Anesthesiologists grades and acute ward length of stay. Limited operating theatre availability was responsible for 60% of delays (96/160), of which 92% (88/96) were considered avoidable. Orthopaedic trauma operating theatre access was compromised (operating theatre unavailable) for 86% of hip fracture surgery delays that were due to limited operating theatre availability. Reasons unrelated to operating theatre availability accounted for 35% of delays (56/160). It was not possible to categorize 5% of delays (8/160).</p><p><strong>Conclusion: </strong>Most hip fracture surgery delays are due to limited operating theatre availability. Of the delays, 78% were considered avoidable, representing a margin for improvement of 55% for operating theatre availability, and 23% unrelated to operating theatre availability.</p>","PeriodicalId":34103,"journal":{"name":"Bone & Joint Open","volume":"6 8","pages":"876-885"},"PeriodicalIF":3.1000,"publicationDate":"2025-08-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12321406/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bone & Joint Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1302/2633-1462.68.BJO-2025-0083.R1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Surgical management of hip fracture is often delayed, which is associated with increased mortality. We aimed to prospectively determine the proportion of potentially avoidable delay to surgery beyond 48 hours, and its causes, as clinically relevant margins for quality improvement.
Methods: A 12-month prospective cohort study from September 2022 to September 2023 was conducted on all 427 hip fracture surgery patients aged ≥ 50 years who were admitted to a trauma centre in New South Wales, Australia. The reasons for delay, medical speciality, and level of seniority initiating the decision, and what response was taken after the delay, were recorded for each case delayed beyond 48 hours from hospital admission. Surgical delays were categorized as either avoidable or unavoidable independently by surgical and medical experts.
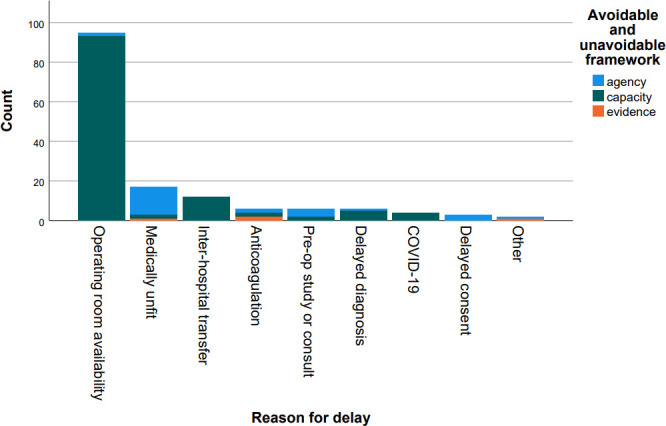
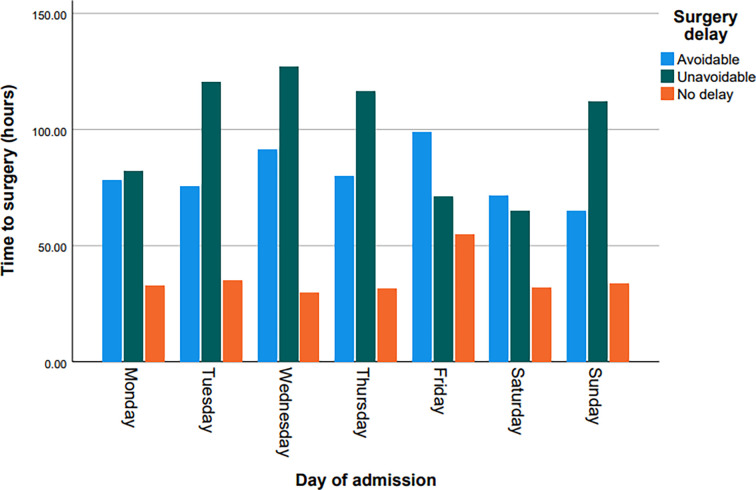
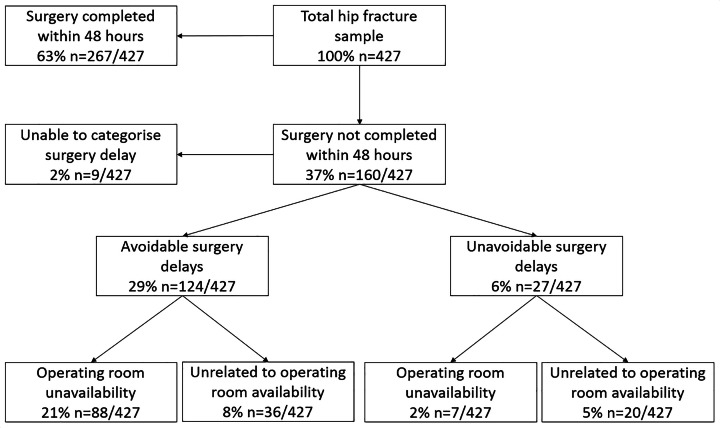
Results: From 427 hip fractures, 37% (160/427) had surgery beyond 48 hours, with 29% (124/427) considered avoidable, 6% (27/427) unavoidable, and 2% (9/427) unable to be categorized. Patients experienced a median 43-hour time to surgery (IQR 27 to 63): 30 hours (IQR 24 to 41) for non-delayed, 69 hours (IQR 55 to 93) for avoidable, and 75 hours (IQR 59 to 135) for unavoidable delays. Patients with unavoidable delays had higher American Society of Anesthesiologists grades and acute ward length of stay. Limited operating theatre availability was responsible for 60% of delays (96/160), of which 92% (88/96) were considered avoidable. Orthopaedic trauma operating theatre access was compromised (operating theatre unavailable) for 86% of hip fracture surgery delays that were due to limited operating theatre availability. Reasons unrelated to operating theatre availability accounted for 35% of delays (56/160). It was not possible to categorize 5% of delays (8/160).
Conclusion: Most hip fracture surgery delays are due to limited operating theatre availability. Of the delays, 78% were considered avoidable, representing a margin for improvement of 55% for operating theatre availability, and 23% unrelated to operating theatre availability.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


