Gabriella B Smith, Nicole S Pham, Amin Alayleh, Stephanie Smith, Karen Chao, Stuart B Goodman, Kevin G Shea
{"title":"Risk Factors for Corticosteroid-associated Osteonecrosis in Children: A National Database Study.","authors":"Gabriella B Smith, Nicole S Pham, Amin Alayleh, Stephanie Smith, Karen Chao, Stuart B Goodman, Kevin G Shea","doi":"10.1016/j.jposna.2025.100199","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Corticosteroid-associated osteonecrosis presents a risk for severe pain and joint collapse. While the relationship between corticosteroid treatment and osteonecrosis in pediatric patients is well-documented, less is known about which patients are at greatest risk across medical conditions. The purpose of this study was to identify high-risk pediatric populations for developing osteonecrosis following corticosteroid treatment across autoimmune, inflammatory, and oncologic conditions.</p><p><strong>Methods: </strong>The Merative MarketScan Research Databases (2007-2022) were queried to identify pediatric patients with an outpatient oral or intravenous corticosteroid prescription. Demographic, clinical, and prescription differences between osteonecrosis and non-osteonecrosis patients were analyzed using t-tests, Fisher's exact, and chi-square tests. Factors associated with time to osteonecrosis were assessed using a multivariable Cox proportional-hazards regression model.</p><p><strong>Results: </strong>We identified 5,606,781 pediatric patients who received corticosteroids, and 131 developed osteonecrosis. The mean time to osteonecrosis following corticosteroid administration was 7.1 months (SD = 5.2). Osteonecrosis patients were significantly older at the age of corticosteroid administration (12.1 [SD = 4.9] vs. 8.2 [5.6], <i>P</i> < .001) and were prescribed corticosteroids for more total days (136.6 [224.8] vs. 17.1 [89.2], <i>P</i> < .001) compared to patients who did not develop osteonecrosis. Adjusting for all other covariates, risk factors for osteonecrosis include acute lymphoblastic leukemia (HR = 575.82, 95% CI = [346.68, 956.40], <i>P</i> < .001), systemic lupus erythematosus (HR = 106.41, 95% CI = [44.65, 253.63], <i>P</i> < .001), Crohn's disease (HR = 6.67, 95% CI = [1.54, 28.86], <i>P</i> = .011), juvenile idiopathic arthritis (HR = 4.62, 95% CI = [1.06, 20.08], <i>P</i> = .041), solid organ transplant (HR = 4.24, 95% CI = [2.08, 8.65], <i>P</i> < .001), dexamethasone (HR = 2.59, 95% CI = [1.56, 4.28], <i>P</i> < .001), older age (hazard ratio [HR] = 1.11, 95% CI = [1.06, 1.16], <i>P</i> < .001), and greater total days prescribed (HR = 1.01, 95% CI = [1.00, 1.02], <i>P</i> = .041).</p><p><strong>Conclusions: </strong>Our national database study highlights the need for targeted screening of pediatric patients treated with high-dose corticosteroids. This investigation may inform multidisciplinary studies and interventions in children treated with corticosteroids.</p><p><strong>Key concepts: </strong>(1)Corticosteroid-associated osteonecrosis presents a risk for severe pain and joint collapse, yet little is known regarding which pediatric patients are at greatest risk across medical conditions.(2)Adjusting for other covariates, pediatric patients with acute lymphoblastic leukemia, systemic lupus erythematous, Crohn's disease, juvenile idiopathic arthritis, solid organ transplants, patients prescribed dexamethasone, patients prescribed corticosteroids for greater total days, and older patients were at increased risk for osteonecrosis in our national database study.(3)Our findings highlight the need for targeted screening of pediatric patients treated with high-dose corticosteroids.(4)Future prospective multidisciplinary screening and intervention protocols should be studied in children treated with corticosteroids.</p><p><strong>Level of evidence: </strong>Level III: Case-control study or retrospective cohort study.</p>","PeriodicalId":520850,"journal":{"name":"Journal of the Pediatric Orthopaedic Society of North America","volume":"12 ","pages":"100199"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12317409/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Pediatric Orthopaedic Society of North America","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/j.jposna.2025.100199","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Corticosteroid-associated osteonecrosis presents a risk for severe pain and joint collapse. While the relationship between corticosteroid treatment and osteonecrosis in pediatric patients is well-documented, less is known about which patients are at greatest risk across medical conditions. The purpose of this study was to identify high-risk pediatric populations for developing osteonecrosis following corticosteroid treatment across autoimmune, inflammatory, and oncologic conditions.
Methods: The Merative MarketScan Research Databases (2007-2022) were queried to identify pediatric patients with an outpatient oral or intravenous corticosteroid prescription. Demographic, clinical, and prescription differences between osteonecrosis and non-osteonecrosis patients were analyzed using t-tests, Fisher's exact, and chi-square tests. Factors associated with time to osteonecrosis were assessed using a multivariable Cox proportional-hazards regression model.
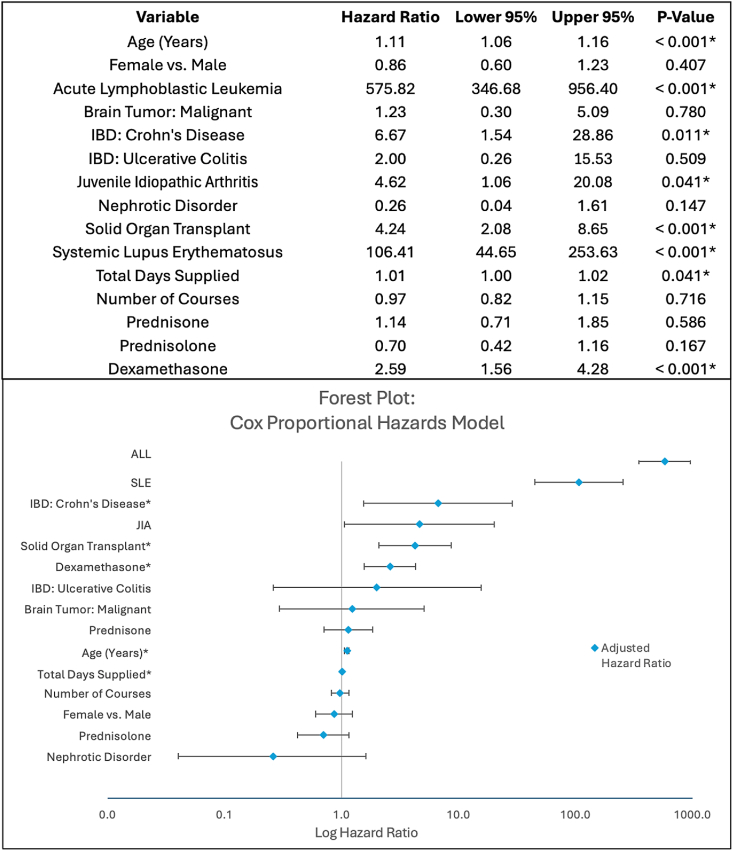
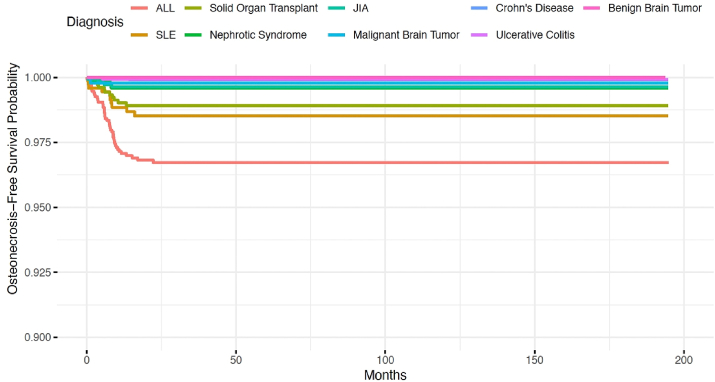
Results: We identified 5,606,781 pediatric patients who received corticosteroids, and 131 developed osteonecrosis. The mean time to osteonecrosis following corticosteroid administration was 7.1 months (SD = 5.2). Osteonecrosis patients were significantly older at the age of corticosteroid administration (12.1 [SD = 4.9] vs. 8.2 [5.6], P < .001) and were prescribed corticosteroids for more total days (136.6 [224.8] vs. 17.1 [89.2], P < .001) compared to patients who did not develop osteonecrosis. Adjusting for all other covariates, risk factors for osteonecrosis include acute lymphoblastic leukemia (HR = 575.82, 95% CI = [346.68, 956.40], P < .001), systemic lupus erythematosus (HR = 106.41, 95% CI = [44.65, 253.63], P < .001), Crohn's disease (HR = 6.67, 95% CI = [1.54, 28.86], P = .011), juvenile idiopathic arthritis (HR = 4.62, 95% CI = [1.06, 20.08], P = .041), solid organ transplant (HR = 4.24, 95% CI = [2.08, 8.65], P < .001), dexamethasone (HR = 2.59, 95% CI = [1.56, 4.28], P < .001), older age (hazard ratio [HR] = 1.11, 95% CI = [1.06, 1.16], P < .001), and greater total days prescribed (HR = 1.01, 95% CI = [1.00, 1.02], P = .041).
Conclusions: Our national database study highlights the need for targeted screening of pediatric patients treated with high-dose corticosteroids. This investigation may inform multidisciplinary studies and interventions in children treated with corticosteroids.
Key concepts: (1)Corticosteroid-associated osteonecrosis presents a risk for severe pain and joint collapse, yet little is known regarding which pediatric patients are at greatest risk across medical conditions.(2)Adjusting for other covariates, pediatric patients with acute lymphoblastic leukemia, systemic lupus erythematous, Crohn's disease, juvenile idiopathic arthritis, solid organ transplants, patients prescribed dexamethasone, patients prescribed corticosteroids for greater total days, and older patients were at increased risk for osteonecrosis in our national database study.(3)Our findings highlight the need for targeted screening of pediatric patients treated with high-dose corticosteroids.(4)Future prospective multidisciplinary screening and intervention protocols should be studied in children treated with corticosteroids.
Level of evidence: Level III: Case-control study or retrospective cohort study.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


