Ashlee J Vance, Clayton J Shuman, Sarah Bell, Anca Tilea, Anna Courant, Karen M Tabb, Kara Zivin
{"title":"Evaluating birthing individual and infant healthcare utilization and costs among individuals experiencing perinatal mood and anxiety disorders.","authors":"Ashlee J Vance, Clayton J Shuman, Sarah Bell, Anca Tilea, Anna Courant, Karen M Tabb, Kara Zivin","doi":"10.1186/s40748-025-00218-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>The maternal-infant connection is fundamental, not only for the psychological wellbeing of both individuals in the dyad, but for their overall health. Yet, their health outcomes are often reported as separate entities. This study offers a novel exploration about how healthcare utilization and costs are interconnected for the dyad. To address this critical gap, our study purpose was to evaluate parallel healthcare utilization outcomes and costs for the birthing person-infant dyad during the postpartum period for those with and without PMAD. The study objectives were to 1) describe healthcare utilization use and costs in the dyad and 2) assess the association of PMAD status with healthcare use and costs in the dyad.</p><p><strong>Objective: </strong>To evaluate parallel healthcare utilization outcomes and costs for the birthing person-infant dyad during the postpartum period for those with and without perinatal mood and anxiety disorders (PMAD).</p><p><strong>Design: </strong>A cross-sectional analysis of healthcare utilization and costs in the postpartum period for birthing individuals and their infants between 2016-2020.</p><p><strong>Setting: </strong>Private insurance data of delivering women in all 50 US states.</p><p><strong>Participants: </strong>The study sample included individuals with evidence of a delivery from 2016 to 2020 who delivered a live singleton newborn. Specifically, we included individuals coded as female, aged 15-44, and with continuous enrollment in a single health plan during the calendar year before and after delivery.</p><p><strong>Results: </strong>The sample consisted of 101,306 birthing individuals and 108,438 infants representing 108,438 unique dyads. Most birthing individuals were between the ages of 25-39 and categorized as White (71.7% of deliveries). Births to White and Black perinatal individuals had the highest percentage with a PMAD diagnosis (21.9% of deliveries to White individuals and 17.9% of deliveries to Black individuals), either in the prenatal or postpartum period. Individuals with pre- or post-delivery PMAD had higher rates of NICU admissions (13.6% and 11.4%, respectively) than those without PMAD (9.9%). Emergency department visits and outpatient utilization decreased over time for both birthing individuals and infants overall. Odds of outpatient services utilization were highest among deliveries with post-PMAD present (newborn Outpatient services aOR: 1.687, CI: 1.274, 2.233 and birthing individual Outpatient services aOR: 6.48, CI: 5.490, 7.648). The PMAD + SUD group had the highest dyadic OOPC (median: $798.32, IQR: $316.20, $1,943.74), and the post-delivery PMAD group had the second highest dyadic costs (median: $505.95, IQR: $211.29, $1,169.01), a difference of almost $300.</p><p><strong>Conclusion: </strong>Results from this study demonstrate significant differences among PMAD groups (i.e., pre-delivery, post-delivery, co-occurring PMAD + SUD) compared to a group without PMAD. This might suggest that PMAD status influences changes in healthcare use or costs. Additionally, the percentage of both birthing individuals and their infants using outpatient services remained nearly identical during the study period, further emphasizing the connection between the dyad and healthcare use.</p>","PeriodicalId":74120,"journal":{"name":"Maternal health, neonatology and perinatology","volume":"11 1","pages":"21"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12320349/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Maternal health, neonatology and perinatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40748-025-00218-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: The maternal-infant connection is fundamental, not only for the psychological wellbeing of both individuals in the dyad, but for their overall health. Yet, their health outcomes are often reported as separate entities. This study offers a novel exploration about how healthcare utilization and costs are interconnected for the dyad. To address this critical gap, our study purpose was to evaluate parallel healthcare utilization outcomes and costs for the birthing person-infant dyad during the postpartum period for those with and without PMAD. The study objectives were to 1) describe healthcare utilization use and costs in the dyad and 2) assess the association of PMAD status with healthcare use and costs in the dyad.
Objective: To evaluate parallel healthcare utilization outcomes and costs for the birthing person-infant dyad during the postpartum period for those with and without perinatal mood and anxiety disorders (PMAD).
Design: A cross-sectional analysis of healthcare utilization and costs in the postpartum period for birthing individuals and their infants between 2016-2020.
Setting: Private insurance data of delivering women in all 50 US states.
Participants: The study sample included individuals with evidence of a delivery from 2016 to 2020 who delivered a live singleton newborn. Specifically, we included individuals coded as female, aged 15-44, and with continuous enrollment in a single health plan during the calendar year before and after delivery.
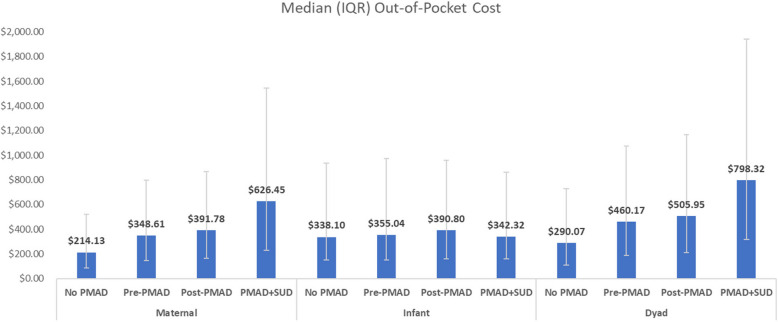
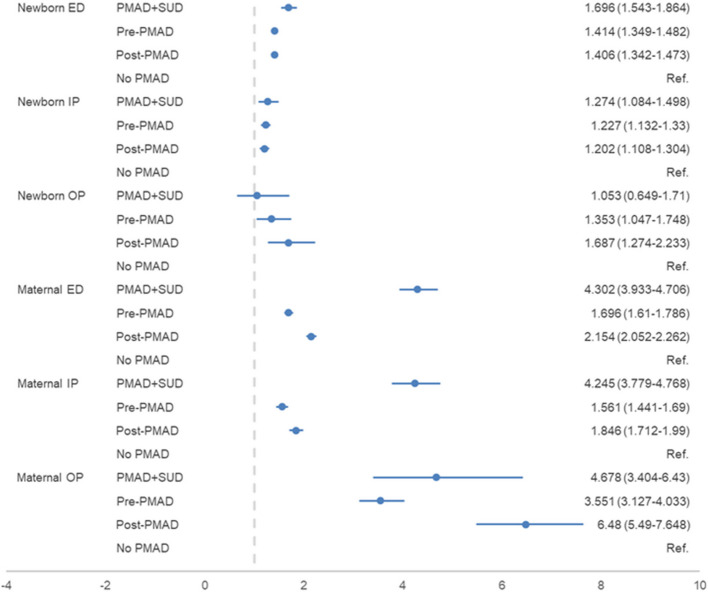
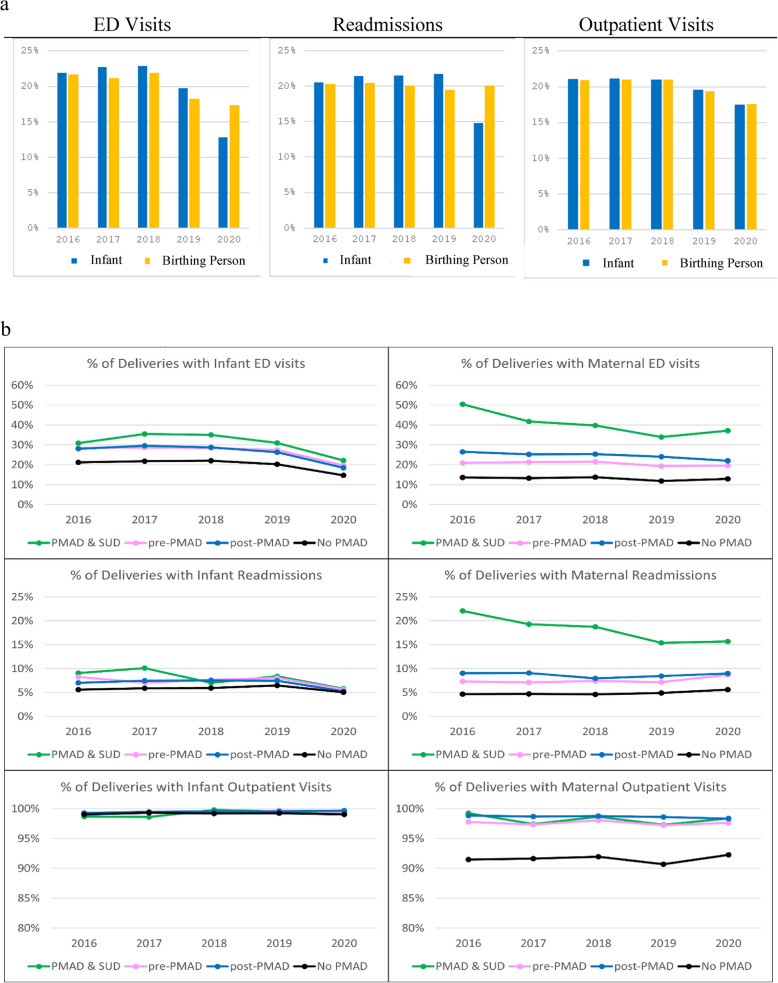
Results: The sample consisted of 101,306 birthing individuals and 108,438 infants representing 108,438 unique dyads. Most birthing individuals were between the ages of 25-39 and categorized as White (71.7% of deliveries). Births to White and Black perinatal individuals had the highest percentage with a PMAD diagnosis (21.9% of deliveries to White individuals and 17.9% of deliveries to Black individuals), either in the prenatal or postpartum period. Individuals with pre- or post-delivery PMAD had higher rates of NICU admissions (13.6% and 11.4%, respectively) than those without PMAD (9.9%). Emergency department visits and outpatient utilization decreased over time for both birthing individuals and infants overall. Odds of outpatient services utilization were highest among deliveries with post-PMAD present (newborn Outpatient services aOR: 1.687, CI: 1.274, 2.233 and birthing individual Outpatient services aOR: 6.48, CI: 5.490, 7.648). The PMAD + SUD group had the highest dyadic OOPC (median: $798.32, IQR: $316.20, $1,943.74), and the post-delivery PMAD group had the second highest dyadic costs (median: $505.95, IQR: $211.29, $1,169.01), a difference of almost $300.
Conclusion: Results from this study demonstrate significant differences among PMAD groups (i.e., pre-delivery, post-delivery, co-occurring PMAD + SUD) compared to a group without PMAD. This might suggest that PMAD status influences changes in healthcare use or costs. Additionally, the percentage of both birthing individuals and their infants using outpatient services remained nearly identical during the study period, further emphasizing the connection between the dyad and healthcare use.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


