Parameter algorithm-driven optimization of surgical approaches: An investigation based on T1 slope minus C2-7 cervical lordosis in patients with cervical degenerative diseases.
Tao Liu, Zhongzheng Zhi, Shuiqiang Qiu, Jian Kang, Jinhao Miao, Zhimin He, Zude Liu
{"title":"Parameter algorithm-driven optimization of surgical approaches: An investigation based on T1 slope minus C2-7 cervical lordosis in patients with cervical degenerative diseases.","authors":"Tao Liu, Zhongzheng Zhi, Shuiqiang Qiu, Jian Kang, Jinhao Miao, Zhimin He, Zude Liu","doi":"10.4103/jcvjs.jcvjs_65_25","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The parameter of T1 slope (T1S) minus C2-7 cervical lordosis (CL) is relevant to the surgical management of cervical degenerative diseases (CDD), but whether it contributes to cervical approaches decision-making has not been reported in the literature prior.</p><p><strong>Purpose: </strong>The purpose of this study was to investigate surgical approach optimization based on T1S minus C2-7 CL in the perioperative management of CDD.</p><p><strong>Materials and methods: </strong>Three hundred sixty-six patients diagnosed with CDD were enrolled from 2018 to 2023. Grouped based on T1S-CL, a value of T1S-CL <20° defined as a matching group, and a value of T1S-CL >20° comprised a matching group. All patients underwent only cervical anterior or posterior approach surgery. Clinical indexes of the Japanese Orthopedic Association (JOA) score, Visual Analog Scale (VAS) and neck disability index (NDI), and radiologic parameters of T1S, CL, and sagittal vertical axis (C2-7 SVA) were recorded and analyzed.</p><p><strong>Results: </strong>Before surgery, there were significant differences in factors between the two groups for CL, T1S, and T1S-CL (<i>P</i> < 0.05). Postoperatively, clinical indexes and radiological parameters changed significantly (<i>P</i> < 0.001) in each group. There are significant correlations indicated between T1S and CL (<i>P</i> < 0.05) except for one in a mismatching group of posterior approach (<i>P</i> > 0.05) postoperatively. There are significant correlations indicated between T1S-CL and T1S, CL (<i>P</i> < 0.05) in two groups of anterior approaches except for posterior approaches (<i>P</i> > 0.05).</p><p><strong>Conclusion: </strong>T1S-CL-based surgical approaches indicate that cervical anterior approaches are superior to posterior paths in improving and optimizing sagittal alignment. Posterior approaches may impair alignment in situations of T1S-CL <20°, and deteriorate malalignment established with conditions of T1S-CL >20°.</p>","PeriodicalId":51721,"journal":{"name":"Journal of Craniovertebral Junction and Spine","volume":"16 2","pages":"180-187"},"PeriodicalIF":1.3000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12313049/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Craniovertebral Junction and Spine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jcvjs.jcvjs_65_25","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/3 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The parameter of T1 slope (T1S) minus C2-7 cervical lordosis (CL) is relevant to the surgical management of cervical degenerative diseases (CDD), but whether it contributes to cervical approaches decision-making has not been reported in the literature prior.
Purpose: The purpose of this study was to investigate surgical approach optimization based on T1S minus C2-7 CL in the perioperative management of CDD.
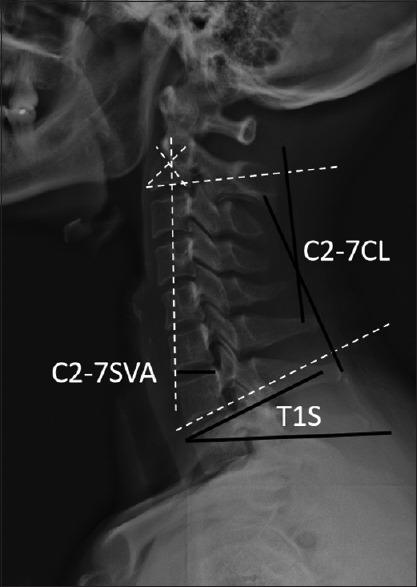
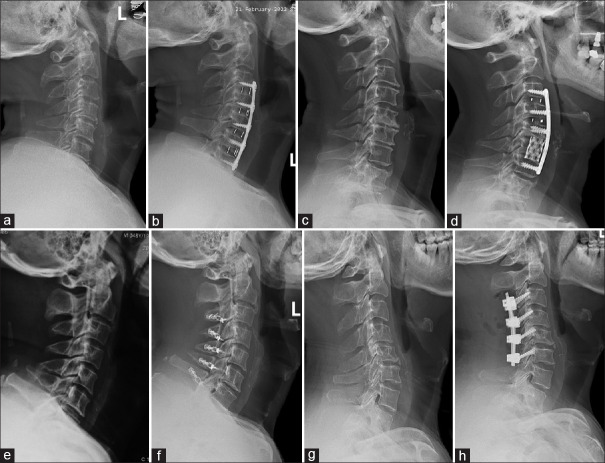
Materials and methods: Three hundred sixty-six patients diagnosed with CDD were enrolled from 2018 to 2023. Grouped based on T1S-CL, a value of T1S-CL <20° defined as a matching group, and a value of T1S-CL >20° comprised a matching group. All patients underwent only cervical anterior or posterior approach surgery. Clinical indexes of the Japanese Orthopedic Association (JOA) score, Visual Analog Scale (VAS) and neck disability index (NDI), and radiologic parameters of T1S, CL, and sagittal vertical axis (C2-7 SVA) were recorded and analyzed.
Results: Before surgery, there were significant differences in factors between the two groups for CL, T1S, and T1S-CL (P < 0.05). Postoperatively, clinical indexes and radiological parameters changed significantly (P < 0.001) in each group. There are significant correlations indicated between T1S and CL (P < 0.05) except for one in a mismatching group of posterior approach (P > 0.05) postoperatively. There are significant correlations indicated between T1S-CL and T1S, CL (P < 0.05) in two groups of anterior approaches except for posterior approaches (P > 0.05).
Conclusion: T1S-CL-based surgical approaches indicate that cervical anterior approaches are superior to posterior paths in improving and optimizing sagittal alignment. Posterior approaches may impair alignment in situations of T1S-CL <20°, and deteriorate malalignment established with conditions of T1S-CL >20°.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


