{"title":"Methotrexate-Associated Hypersensitivity Pneumonitis After 15 Years of Use: A Case Report and Literature Review.","authors":"Dilara Bulut Gökten, Rıdvan Mercan","doi":"10.31138/mjr.080225.arc","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This report presents a case of methotrexate (MTX)-associated hypersensitivity pneumonitis (HP) after 15 years of use and reviews the literature on its diagnosis, treatment, symptoms, and risk factors.</p><p><strong>Case: </strong>A 65-year-old female patient with rheumatoid arthritis (RA) presented with shortness of breath and a non-productive cough after 15 years of stable MTX treatment. Chest X-ray revealed bilateral ill-defined infiltrates, and high-resolution computed tomography (HRCT) showed diffuse ground-glass opacities. All diagnostic tests for infection were negative. Suspecting MTX-associated HP, MTX was discontinued, leading to significant clinical improvement.</p><p><strong>Discussion: </strong>HP is the most common form of pulmonary toxicity associated with MTX. Symptoms typically include dry cough and dyspnoea in 80% of patients. Significant eosinophilia may be observed. Risk factors include age over 60, diabetes, pre-existing lung disease, hypoalbuminemia, RA-related lung involvement, renal dysfunction, male gender, and Daily dose. The diagnosis of MTX-associated HP is a diagnosis of exclusion. Differential diagnosis can be challenging, as it may overlap with other conditions. Although diagnostic criteria have been reported, diagnosis is primarily based on clinical, radiological, and laboratory findings, along with treatment response. Management involves discontinuation of MTX and corticosteroid therapy. While MTX-associated HP generally follows a favourable course with most patients achieving full recovery, reported mortality rates can be as high as 17.6%.</p><p><strong>Conclusion: </strong>While MTX-associated HP is usually reported within the first years of treatment, it can also occur after prolonged use. Clinicians should consider this possibility in the differential diagnosis, as early detection can result in treatable outcomes.</p>","PeriodicalId":32816,"journal":{"name":"Mediterranean Journal of Rheumatology","volume":"36 2","pages":"316-321"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12312479/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mediterranean Journal of Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31138/mjr.080225.arc","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: This report presents a case of methotrexate (MTX)-associated hypersensitivity pneumonitis (HP) after 15 years of use and reviews the literature on its diagnosis, treatment, symptoms, and risk factors.
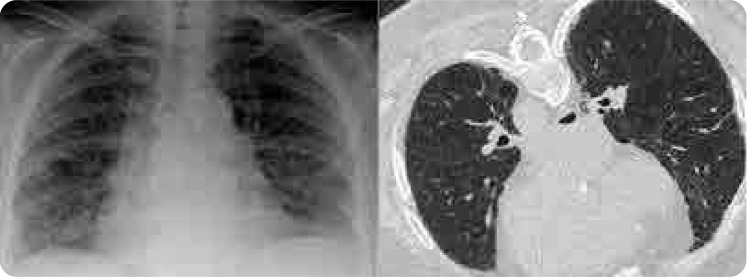
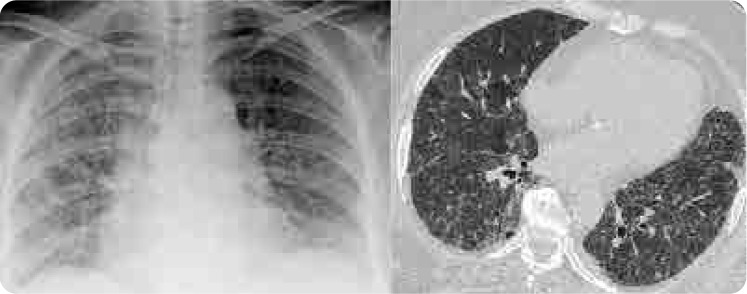
Case: A 65-year-old female patient with rheumatoid arthritis (RA) presented with shortness of breath and a non-productive cough after 15 years of stable MTX treatment. Chest X-ray revealed bilateral ill-defined infiltrates, and high-resolution computed tomography (HRCT) showed diffuse ground-glass opacities. All diagnostic tests for infection were negative. Suspecting MTX-associated HP, MTX was discontinued, leading to significant clinical improvement.
Discussion: HP is the most common form of pulmonary toxicity associated with MTX. Symptoms typically include dry cough and dyspnoea in 80% of patients. Significant eosinophilia may be observed. Risk factors include age over 60, diabetes, pre-existing lung disease, hypoalbuminemia, RA-related lung involvement, renal dysfunction, male gender, and Daily dose. The diagnosis of MTX-associated HP is a diagnosis of exclusion. Differential diagnosis can be challenging, as it may overlap with other conditions. Although diagnostic criteria have been reported, diagnosis is primarily based on clinical, radiological, and laboratory findings, along with treatment response. Management involves discontinuation of MTX and corticosteroid therapy. While MTX-associated HP generally follows a favourable course with most patients achieving full recovery, reported mortality rates can be as high as 17.6%.
Conclusion: While MTX-associated HP is usually reported within the first years of treatment, it can also occur after prolonged use. Clinicians should consider this possibility in the differential diagnosis, as early detection can result in treatable outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


