Komal Abdul Rahim, Bilal Ahmed Usmani, Syed Iqbal Azam, Saad Bin Zafar Mahmood, Mushyada Ali, Anum Rahim, Imran Nisar, Zainab Samad, Adil H Haider
{"title":"Infections do not play fair: the Charlson-Age Comorbidity Index reveals sex-specific risk in laparotomy patients in an LMIC.","authors":"Komal Abdul Rahim, Bilal Ahmed Usmani, Syed Iqbal Azam, Saad Bin Zafar Mahmood, Mushyada Ali, Anum Rahim, Imran Nisar, Zainab Samad, Adil H Haider","doi":"10.1136/tsaco-2024-001659","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Surgical site infections (SSIs) are a major cause of increased morbidity, hospital stay, care costs, and mortality in surgical patients; these can be prognosticated by the Charlson Comorbidity Index (CCI) and accounting for age-the Charlson-Age Comorbidity Index (CACI). Given the limited use of CCI/CACI in low- and middle-income countries, we aimed to assess the use of CCI/CACI in prognosticating the 30-day incidence of SSIs among exploratory laparotomy patients at a tertiary care center in Pakistan.</p><p><strong>Methods: </strong>The study analyzed data from adult patients with International Classification of Diseases-9 CM primary index procedure codes for exploratory laparotomy at a tertiary teaching hospital between 2010 and 2019. The primary exposure was categorized into mild (score 1-2), moderate (score 3-4), and severe (score >5) based on CCI/CACI. The outcome of interest was the incidence of SSIs, where days after operation were restricted to 30 days or less within a hospital stay. Adjusted ORs (AOR) with 95% CI are reported using multiple logistic regression.</p><p><strong>Results: </strong>Out of 2,267 exploratory laparotomy patients, 54.43% were classified as having comorbidity. There was no difference noted in the incidence of SSIs among no CACI (15.88%) and patients with mild, moderate, and severe CACI (18.49%, 18.94%, and 17.42%). Effect modification showed that, among females, CCI/CACI was not significantly associated with SSIs but showed a significant association in males. Among males, a dose-response relationship was observed, with severe CACI having the highest odds of developing SSIs (AOR 2.04; 95% CI 1.35 to 3.05) compared with patients with no CACI. Subgroup analysis yielded similar results (AOR 2.03; 95% CI 1.28 to 3.21).</p><p><strong>Conclusion: </strong>Findings suggested that the comorbidity index is valuable in prognosticating surgical outcomes in exploratory laparotomy patients among males, with age being an integral part of the index. CACI should be calculated for risk stratification and management purposes in male patients undergoing exploratory laparotomy.</p><p><strong>Level of evidence: </strong>III.</p>","PeriodicalId":23307,"journal":{"name":"Trauma Surgery & Acute Care Open","volume":"10 2","pages":"e001659"},"PeriodicalIF":2.2000,"publicationDate":"2025-06-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12314809/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Trauma Surgery & Acute Care Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/tsaco-2024-001659","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Surgical site infections (SSIs) are a major cause of increased morbidity, hospital stay, care costs, and mortality in surgical patients; these can be prognosticated by the Charlson Comorbidity Index (CCI) and accounting for age-the Charlson-Age Comorbidity Index (CACI). Given the limited use of CCI/CACI in low- and middle-income countries, we aimed to assess the use of CCI/CACI in prognosticating the 30-day incidence of SSIs among exploratory laparotomy patients at a tertiary care center in Pakistan.
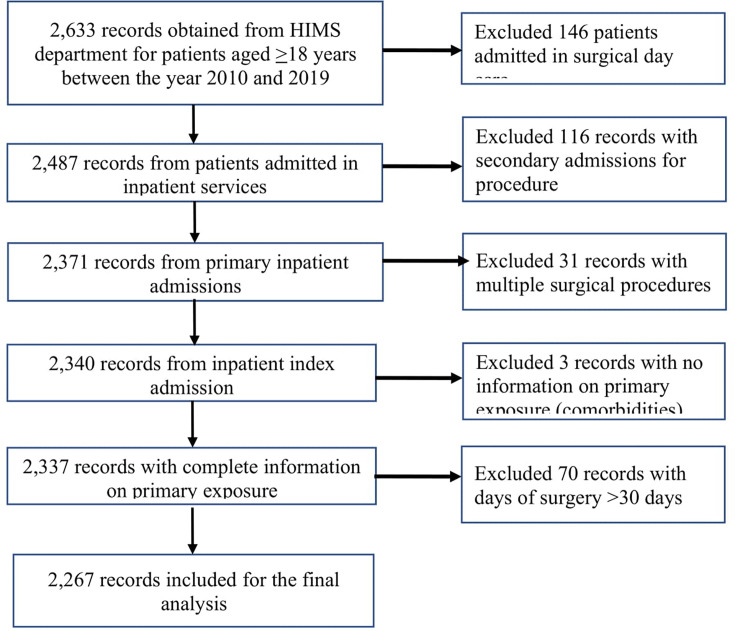
Methods: The study analyzed data from adult patients with International Classification of Diseases-9 CM primary index procedure codes for exploratory laparotomy at a tertiary teaching hospital between 2010 and 2019. The primary exposure was categorized into mild (score 1-2), moderate (score 3-4), and severe (score >5) based on CCI/CACI. The outcome of interest was the incidence of SSIs, where days after operation were restricted to 30 days or less within a hospital stay. Adjusted ORs (AOR) with 95% CI are reported using multiple logistic regression.
Results: Out of 2,267 exploratory laparotomy patients, 54.43% were classified as having comorbidity. There was no difference noted in the incidence of SSIs among no CACI (15.88%) and patients with mild, moderate, and severe CACI (18.49%, 18.94%, and 17.42%). Effect modification showed that, among females, CCI/CACI was not significantly associated with SSIs but showed a significant association in males. Among males, a dose-response relationship was observed, with severe CACI having the highest odds of developing SSIs (AOR 2.04; 95% CI 1.35 to 3.05) compared with patients with no CACI. Subgroup analysis yielded similar results (AOR 2.03; 95% CI 1.28 to 3.21).
Conclusion: Findings suggested that the comorbidity index is valuable in prognosticating surgical outcomes in exploratory laparotomy patients among males, with age being an integral part of the index. CACI should be calculated for risk stratification and management purposes in male patients undergoing exploratory laparotomy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


