Management of critically located brain metastases in patients with precluded survival using customised double-dose prescription-based, adaptive accelerated staged radiosurgery: a long-term retrospective analysis.
G Sinclair, H Martin, C M Allison, M A Hatiboglu, H Speckter, A Fytagoridis
{"title":"Management of critically located brain metastases in patients with precluded survival using customised double-dose prescription-based, adaptive accelerated staged radiosurgery: a long-term retrospective analysis.","authors":"G Sinclair, H Martin, C M Allison, M A Hatiboglu, H Speckter, A Fytagoridis","doi":"10.1186/s13014-025-02692-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with brain metastases face a poor prognosis when deemed not to be suitable for onco-surgical intervention. This feasibility study analyses the outcome of adaptive radiosurgery applied in customised settings to a group of patients with brain metastases, where no other form of treatment was deemed safe and/or feasible.</p><p><strong>Methods: </strong>29 patients with 35 brain metastases deemed not to be candidates for surgery, radiotherapy or systemic treatment were treated with MRI-guided adaptive Gamma Knife radiosurgery in 3 separate sessions with a 72-hour interval. Customised synchronous double-dose prescriptions were systematically utilised at each session. Estimated survival at pre-treatment was fewer than 4 weeks due to the targeted intracranial lesions. A retrospective analysis was conducted on the whole cohort, with particular emphasis on those surviving 12 months and beyond.</p><p><strong>Results: </strong>The median overall survival was 7.3 months, with a follow-up of 7.5 years. Survival at 6, 12, 24, 36, 48 and 60 months was 62%, 41%, 17%, 14%, 10% and 7%, respectively. Local tumour control (LTC) at 1 year was 75%. 4 patients developed local recurrence late on follow-up, with a survival ranging between 12 and 40 months. 2 patients were alive at the time of submission (115- and 117-months post-treatment) with no sequelae; the remainder succumbed to general disease progression, with neurologic death being avoided throughout the whole cohort. Adverse radiation effects (ARE) were reported in 5 patients, of which 4 remained asymptomatic throughout follow-up.</p><p><strong>Conclusions: </strong>Based on the results of this first retrospective study, adaptive radiosurgery in double-dose prescription settings provided acceptable rates of LTC and ARE despite the underlying accelerated timeline, ultimately preventing neurologic death in a group of patients with an extremely poor prognosis. Prospective studies involving a larger number of patients with homogenous histology are warranted to validate the results of this study and optimise the technique.</p>","PeriodicalId":49639,"journal":{"name":"Radiation Oncology","volume":"20 1","pages":"120"},"PeriodicalIF":3.3000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12317634/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13014-025-02692-x","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patients with brain metastases face a poor prognosis when deemed not to be suitable for onco-surgical intervention. This feasibility study analyses the outcome of adaptive radiosurgery applied in customised settings to a group of patients with brain metastases, where no other form of treatment was deemed safe and/or feasible.
Methods: 29 patients with 35 brain metastases deemed not to be candidates for surgery, radiotherapy or systemic treatment were treated with MRI-guided adaptive Gamma Knife radiosurgery in 3 separate sessions with a 72-hour interval. Customised synchronous double-dose prescriptions were systematically utilised at each session. Estimated survival at pre-treatment was fewer than 4 weeks due to the targeted intracranial lesions. A retrospective analysis was conducted on the whole cohort, with particular emphasis on those surviving 12 months and beyond.
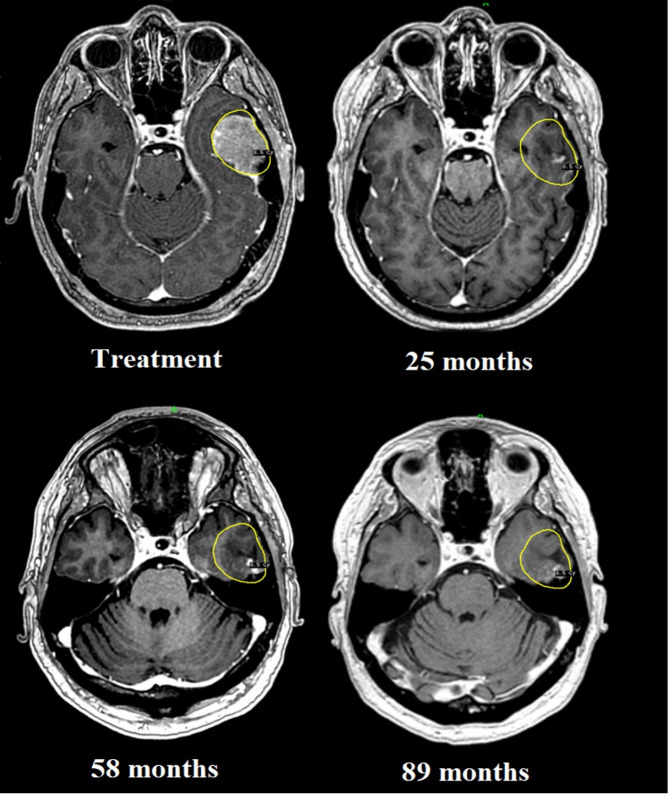
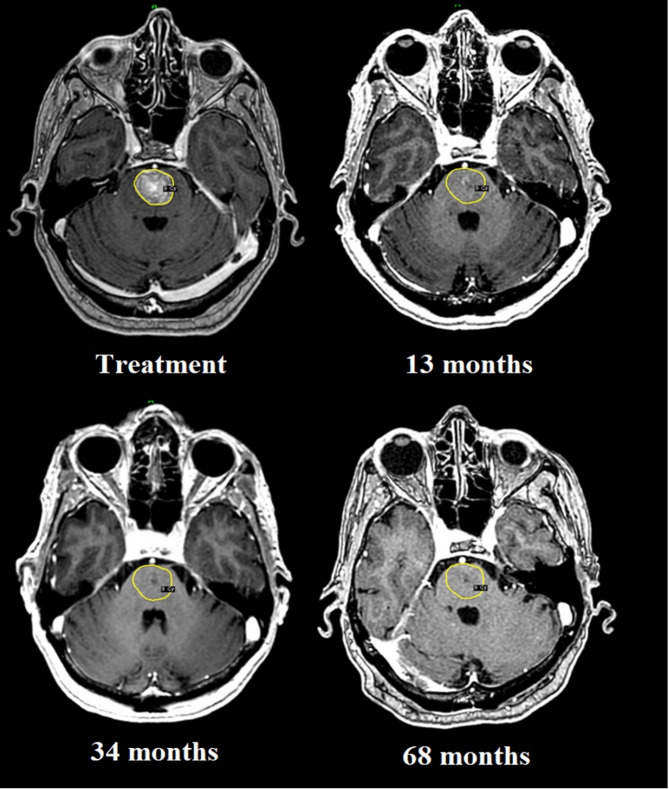
Results: The median overall survival was 7.3 months, with a follow-up of 7.5 years. Survival at 6, 12, 24, 36, 48 and 60 months was 62%, 41%, 17%, 14%, 10% and 7%, respectively. Local tumour control (LTC) at 1 year was 75%. 4 patients developed local recurrence late on follow-up, with a survival ranging between 12 and 40 months. 2 patients were alive at the time of submission (115- and 117-months post-treatment) with no sequelae; the remainder succumbed to general disease progression, with neurologic death being avoided throughout the whole cohort. Adverse radiation effects (ARE) were reported in 5 patients, of which 4 remained asymptomatic throughout follow-up.
Conclusions: Based on the results of this first retrospective study, adaptive radiosurgery in double-dose prescription settings provided acceptable rates of LTC and ARE despite the underlying accelerated timeline, ultimately preventing neurologic death in a group of patients with an extremely poor prognosis. Prospective studies involving a larger number of patients with homogenous histology are warranted to validate the results of this study and optimise the technique.
Radiation OncologyONCOLOGY-RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING
CiteScore
6.50
自引率
2.80%
发文量
181
审稿时长
3-6 weeks
期刊介绍:
Radiation Oncology encompasses all aspects of research that impacts on the treatment of cancer using radiation. It publishes findings in molecular and cellular radiation biology, radiation physics, radiation technology, and clinical oncology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


