{"title":"The role of vital signs in predicting mortality risk in elderly patients visiting the emergency department.","authors":"Karin Erwander, Björn Agvall, Kjell Ivarsson","doi":"10.1186/s12873-025-01307-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Accurate risk stratification in older adults presenting to the emergency department (ED) is essential but challenging due to atypical presentations and age-related physiological changes. While vital signs are central to triage, their predictive value for short-term mortality in this population remains unclear. This study aimed to explore the association between initial vital signs and 7-day mortality among older ED patients.</p><p><strong>Method: </strong>This retrospective cohort study included patients aged ≥ 65 years who visited two EDs in Region Halland, Sweden, during 2018. Vital signs, systolic blood pressure (SBP), heart rate (HR), peripheral oxygen saturation (SpO₂), respiratory rate (RR), body temperature, and level of consciousness (LOC), were extracted from the regional health information system. Descriptive statistics, ROC curve analysis, and logistic regression were used to assess associations between categorized vital signs and 7-day mortality, adjusting for age, sex, and comorbidity.</p><p><strong>Results: </strong>Of 30 327 ED visits, 25 450 patients had at least one recorded vital sign. The mean age was 78 years; 50% were female. The 7-day mortality rate was 2%. ROC analysis showed limited discriminative ability of individual vital signs (AUC range: 0.49-0.70). Low SBP, high HR, low SpO₂, and impaired LOC were statistically significantly associated with mortality. Multivariable logistic regression confirmed these associations, with SBP (≤ 80 mmHg, AOR 7.79; 95% CI 3.27-18.54), high HR (> 125 bpm, AOR 6.37; 95% CI 1.26-32.16), low SpO₂ (≤ 80%, AOR 3.64; 95% CI 1.75-7.58), and impaired LOC (GCS < 13 (AOR 9.30-18.36)) showing the strongest effects.</p><p><strong>Conclusion: </strong>Low SBP, elevated HR, reduced SpO₂, and impaired LOC were independently associated with short-term mortality in older ED patients, though their individual predictive performance was modest. LOC, despite being a strong predictor, was frequently missing, underscoring challenges in routine assessment. These findings highlight the need for more comprehensive, geriatric-informed triage systems that incorporate age-related physiological changes and ensure consistent evaluation of LOC. As frailty and functional status was not available in this dataset, future studies should focus on integrated models that include these factors to improve early risk identification in emergency care for older adults.</p><p><strong>Clinical trial number: </strong>Not applicable.</p>","PeriodicalId":9002,"journal":{"name":"BMC Emergency Medicine","volume":"25 1","pages":"144"},"PeriodicalIF":2.3000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12317628/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12873-025-01307-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Accurate risk stratification in older adults presenting to the emergency department (ED) is essential but challenging due to atypical presentations and age-related physiological changes. While vital signs are central to triage, their predictive value for short-term mortality in this population remains unclear. This study aimed to explore the association between initial vital signs and 7-day mortality among older ED patients.
Method: This retrospective cohort study included patients aged ≥ 65 years who visited two EDs in Region Halland, Sweden, during 2018. Vital signs, systolic blood pressure (SBP), heart rate (HR), peripheral oxygen saturation (SpO₂), respiratory rate (RR), body temperature, and level of consciousness (LOC), were extracted from the regional health information system. Descriptive statistics, ROC curve analysis, and logistic regression were used to assess associations between categorized vital signs and 7-day mortality, adjusting for age, sex, and comorbidity.
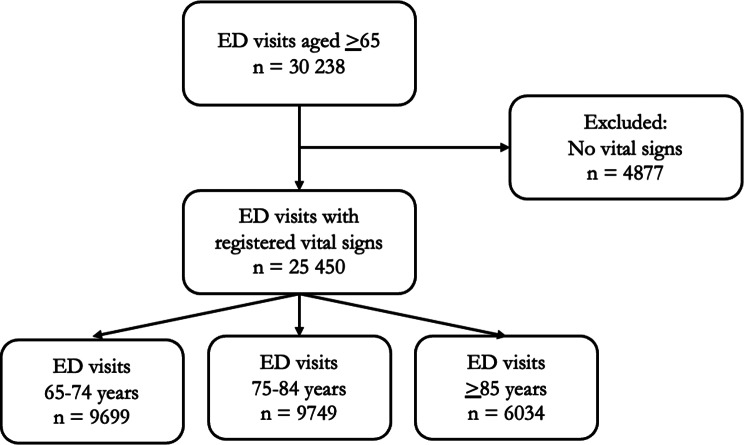
Results: Of 30 327 ED visits, 25 450 patients had at least one recorded vital sign. The mean age was 78 years; 50% were female. The 7-day mortality rate was 2%. ROC analysis showed limited discriminative ability of individual vital signs (AUC range: 0.49-0.70). Low SBP, high HR, low SpO₂, and impaired LOC were statistically significantly associated with mortality. Multivariable logistic regression confirmed these associations, with SBP (≤ 80 mmHg, AOR 7.79; 95% CI 3.27-18.54), high HR (> 125 bpm, AOR 6.37; 95% CI 1.26-32.16), low SpO₂ (≤ 80%, AOR 3.64; 95% CI 1.75-7.58), and impaired LOC (GCS < 13 (AOR 9.30-18.36)) showing the strongest effects.
Conclusion: Low SBP, elevated HR, reduced SpO₂, and impaired LOC were independently associated with short-term mortality in older ED patients, though their individual predictive performance was modest. LOC, despite being a strong predictor, was frequently missing, underscoring challenges in routine assessment. These findings highlight the need for more comprehensive, geriatric-informed triage systems that incorporate age-related physiological changes and ensure consistent evaluation of LOC. As frailty and functional status was not available in this dataset, future studies should focus on integrated models that include these factors to improve early risk identification in emergency care for older adults.
期刊介绍:
BMC Emergency Medicine is an open access, peer-reviewed journal that considers articles on all urgent and emergency aspects of medicine, in both practice and basic research. In addition, the journal covers aspects of disaster medicine and medicine in special locations, such as conflict areas and military medicine, together with articles concerning healthcare services in the emergency departments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


