Nadeev Wijesuriya, Helen Sinabulya, Helena Johann-Meyer, Keisha Kellman, Felicity de Vere, Sandra Howell, Alphonsus Liew, Paolo Bosco, Steven A Niederer, Stephen Black, Christopher A Rinaldi
{"title":"Joint Pacing and Vascular Intervention for the Management of Cardiac Device Associated Central Venous Obstruction.","authors":"Nadeev Wijesuriya, Helen Sinabulya, Helena Johann-Meyer, Keisha Kellman, Felicity de Vere, Sandra Howell, Alphonsus Liew, Paolo Bosco, Steven A Niederer, Stephen Black, Christopher A Rinaldi","doi":"10.1111/pace.70019","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>Central venous obstruction (CVO) increases the complexity of pacing interventions, whether it be with device-associated symptomatic superior vena cava syndrome (SVCS), or by impeding new implants. Endovascular treatment involves the joint expertise of both cardiac pacing and vascular specialists. We report the outcomes of such procedures at our institution.</p><p><strong>Methods: </strong>A single-center retrospective observational study, examining outcomes of joint pacing-vascular procedures for CVO. Cases were screened from an existing institutional database.</p><p><strong>Results: </strong>There were 19 total cases. Two were new device implants where the novel \"inside-out\" procedure was utilized to establish access in SVCS, both with no complications. The remainder (n = 17) were transvenous lead extractions plus attempted recanalization of CVO using venoplasty with or without stenting. Transvenous devices were re-implanted in eight patients. Complete procedure success rate was 84%. There were two cases of pericardial effusion requiring pericardiocentesis, resulting in procedure abandonment. There was no in-hospital mortality and no cases of emergency sternotomy. Over mean follow-up of 28 months, 2/6 patients receiving venoplasty (33%) and 2/8 patients receiving stenting (25%) required re-intervention for symptomatic restenosis. Of the patients who were not re-implanted with a transvenous device following initially successful endovascular intervention (6/14), none had recurrence over the follow-up period.</p><p><strong>Conclusion: </strong>Pacing interventions in SVCS carry a significant risk profile, requiring management by experienced operators in high-volume centers to maximize safety. Endovascular interventions have a significant recurrence rate, with up-front stenting potentially being superior. Our data suggests that those without re-implantation of transvenous leads may have better long term outcomes.</p>","PeriodicalId":520740,"journal":{"name":"Pacing and clinical electrophysiology : PACE","volume":" ","pages":"959-966"},"PeriodicalIF":1.3000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12439234/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pacing and clinical electrophysiology : PACE","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1111/pace.70019","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background and aims: Central venous obstruction (CVO) increases the complexity of pacing interventions, whether it be with device-associated symptomatic superior vena cava syndrome (SVCS), or by impeding new implants. Endovascular treatment involves the joint expertise of both cardiac pacing and vascular specialists. We report the outcomes of such procedures at our institution.
Methods: A single-center retrospective observational study, examining outcomes of joint pacing-vascular procedures for CVO. Cases were screened from an existing institutional database.
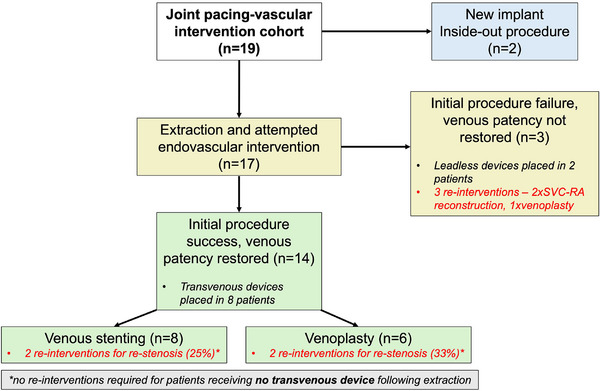
Results: There were 19 total cases. Two were new device implants where the novel "inside-out" procedure was utilized to establish access in SVCS, both with no complications. The remainder (n = 17) were transvenous lead extractions plus attempted recanalization of CVO using venoplasty with or without stenting. Transvenous devices were re-implanted in eight patients. Complete procedure success rate was 84%. There were two cases of pericardial effusion requiring pericardiocentesis, resulting in procedure abandonment. There was no in-hospital mortality and no cases of emergency sternotomy. Over mean follow-up of 28 months, 2/6 patients receiving venoplasty (33%) and 2/8 patients receiving stenting (25%) required re-intervention for symptomatic restenosis. Of the patients who were not re-implanted with a transvenous device following initially successful endovascular intervention (6/14), none had recurrence over the follow-up period.
Conclusion: Pacing interventions in SVCS carry a significant risk profile, requiring management by experienced operators in high-volume centers to maximize safety. Endovascular interventions have a significant recurrence rate, with up-front stenting potentially being superior. Our data suggests that those without re-implantation of transvenous leads may have better long term outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


