Eran Politzer, Timothy S Anderson, John Z Ayanian, Vilsa E Curto, Jeffrey Souza, Thomas C Tsai, Bruce E Landon
{"title":"Perioperative Costs of Elective Surgical Procedures in Medicare Advantage Compared With Traditional Medicare.","authors":"Eran Politzer, Timothy S Anderson, John Z Ayanian, Vilsa E Curto, Jeffrey Souza, Thomas C Tsai, Bruce E Landon","doi":"10.1001/jamahealthforum.2025.2258","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>The utilization of elective surgical procedures is lower for patients enrolled in Medicare Advantage (MA) than in traditional Medicare (TM), but it remains unclear whether surgical episode costs differ between MA and TM for comparable patients.</p><p><strong>Objective: </strong>To compare the estimated costs, markers of resource use (eg, length of stay and location of surgery), and outcomes of surgical episodes for similar patients enrolled in MA and TM.</p><p><strong>Design, setting, and participants: </strong>In this retrospective cohort study, 2019 Medicare claims and encounters data were analyzed to compare differences in surgical episode costs for beneficiaries with MA vs TM who underwent common elective surgical procedures across 11 categories. Procedures performed in either inpatient or outpatient settings were included in the analysis. Data were analyzed from January 2023 to March 2025.</p><p><strong>Exposures: </strong>Enrollment in MA or TM.</p><p><strong>Main outcomes and measures: </strong>The primary outcomes were estimated 30-day costs of surgical episodes and factors affecting costs and/or outcomes, including share of inpatient procedures, length of stay, share of patients discharged home, and 30-day readmission rates. A secondary outcome explored potential facility selection and patient steering by estimating the distance traveled to surgery. Multivariable linear regression models adjusted for the type of surgical procedure, patient characteristics, and their Elixhauser Comorbidity Index were used to compare outcomes of surgical episodes in patients with MA vs TM within hospital referral regions.</p><p><strong>Results: </strong>The analysis included 1 177 700 surgical procedures among 1 110 263 Medicare beneficiaries (mean [SD] age, 73.42 [5.8] years; 686 708 females [58.3%]). The overall rate of surgery utilization was lower among MA patients vs TM patients (difference in rate, -4.4%; 95% CI, -4.8% to -4.1%), with variation found across surgical categories. Across procedures, 30-day surgical episode costs for MA patients vs TM patients were, on average, $671 (95% CI, $639-$702) lower. The share of procedures billed at the higher inpatient rate was 5.41 (95% CI, 5.23-5.58) percentage points (pp) lower for MA patients than for TM patients, and the mean length of inpatient stay was 0.27 (95% CI, 0.26-0.29) days shorter. The share of patients discharged home was higher for those with MA vs TM (3.82 [95% CI, 3.65-3.99] pp). MA patients traveled a mean of 2.32 (95% CI, 1.62-3.01) miles farther for surgery. Readmission rates were lower for patients with MA (-0.70 [95% CI, -0.83 to -0.58] pp).</p><p><strong>Conclusions and relevance: </strong>This study found that in addition to lower utilization of common elective surgical procedures, the costs of surgical episodes were lower for patients enrolled in MA than those enrolled in TM. MA plans had lower costs because more procedures were performed in outpatient settings, required shorter lengths of stay, and less expensive postacute care, with no apparent harm to overall quality. Physician and surgical facility selection and patient steering likely contributed to these cost differences. These findings highlight potential mechanisms by which MA plans may achieve cost savings compared with TM plans.</p>","PeriodicalId":53180,"journal":{"name":"JAMA Health Forum","volume":"6 8","pages":"e252258"},"PeriodicalIF":11.3000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12317349/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Health Forum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1001/jamahealthforum.2025.2258","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: The utilization of elective surgical procedures is lower for patients enrolled in Medicare Advantage (MA) than in traditional Medicare (TM), but it remains unclear whether surgical episode costs differ between MA and TM for comparable patients.
Objective: To compare the estimated costs, markers of resource use (eg, length of stay and location of surgery), and outcomes of surgical episodes for similar patients enrolled in MA and TM.
Design, setting, and participants: In this retrospective cohort study, 2019 Medicare claims and encounters data were analyzed to compare differences in surgical episode costs for beneficiaries with MA vs TM who underwent common elective surgical procedures across 11 categories. Procedures performed in either inpatient or outpatient settings were included in the analysis. Data were analyzed from January 2023 to March 2025.
Exposures: Enrollment in MA or TM.
Main outcomes and measures: The primary outcomes were estimated 30-day costs of surgical episodes and factors affecting costs and/or outcomes, including share of inpatient procedures, length of stay, share of patients discharged home, and 30-day readmission rates. A secondary outcome explored potential facility selection and patient steering by estimating the distance traveled to surgery. Multivariable linear regression models adjusted for the type of surgical procedure, patient characteristics, and their Elixhauser Comorbidity Index were used to compare outcomes of surgical episodes in patients with MA vs TM within hospital referral regions.
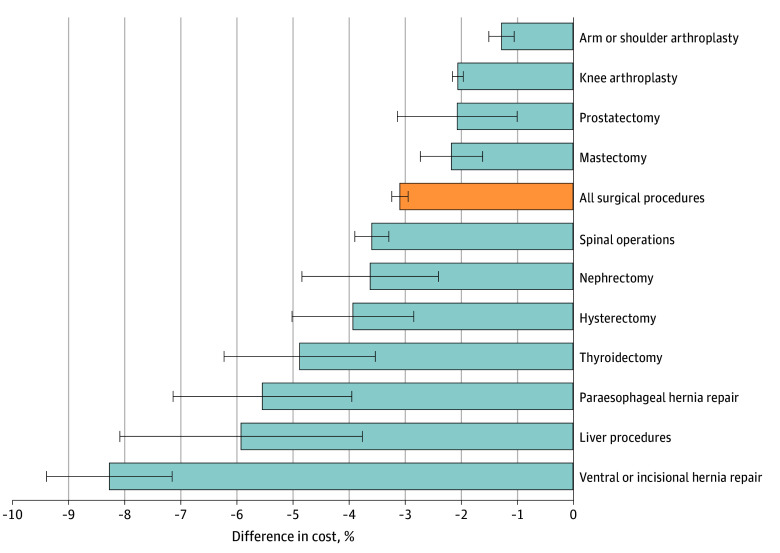
Results: The analysis included 1 177 700 surgical procedures among 1 110 263 Medicare beneficiaries (mean [SD] age, 73.42 [5.8] years; 686 708 females [58.3%]). The overall rate of surgery utilization was lower among MA patients vs TM patients (difference in rate, -4.4%; 95% CI, -4.8% to -4.1%), with variation found across surgical categories. Across procedures, 30-day surgical episode costs for MA patients vs TM patients were, on average, $671 (95% CI, $639-$702) lower. The share of procedures billed at the higher inpatient rate was 5.41 (95% CI, 5.23-5.58) percentage points (pp) lower for MA patients than for TM patients, and the mean length of inpatient stay was 0.27 (95% CI, 0.26-0.29) days shorter. The share of patients discharged home was higher for those with MA vs TM (3.82 [95% CI, 3.65-3.99] pp). MA patients traveled a mean of 2.32 (95% CI, 1.62-3.01) miles farther for surgery. Readmission rates were lower for patients with MA (-0.70 [95% CI, -0.83 to -0.58] pp).
Conclusions and relevance: This study found that in addition to lower utilization of common elective surgical procedures, the costs of surgical episodes were lower for patients enrolled in MA than those enrolled in TM. MA plans had lower costs because more procedures were performed in outpatient settings, required shorter lengths of stay, and less expensive postacute care, with no apparent harm to overall quality. Physician and surgical facility selection and patient steering likely contributed to these cost differences. These findings highlight potential mechanisms by which MA plans may achieve cost savings compared with TM plans.
期刊介绍:
JAMA Health Forum is an international, peer-reviewed, online, open access journal that addresses health policy and strategies affecting medicine, health, and health care. The journal publishes original research, evidence-based reports, and opinion about national and global health policy. It covers innovative approaches to health care delivery and health care economics, access, quality, safety, equity, and reform.
In addition to publishing articles, JAMA Health Forum also features commentary from health policy leaders on the JAMA Forum. It covers news briefs on major reports released by government agencies, foundations, health policy think tanks, and other policy-focused organizations.
JAMA Health Forum is a member of the JAMA Network, which is a consortium of peer-reviewed, general medical and specialty publications. The journal presents curated health policy content from across the JAMA Network, including journals such as JAMA and JAMA Internal Medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


