Midterm Outcomes of Pediatric Mitral Valvuloplasty for Moderate to Severe Mitral Valve Regurgitation and Associated Risk Factors for Postoperative Deterioration.
Hongyuan Fu, Aijun Liu, Ming Yang, Zeyu Liu, Junwu Su
{"title":"Midterm Outcomes of Pediatric Mitral Valvuloplasty for Moderate to Severe Mitral Valve Regurgitation and Associated Risk Factors for Postoperative Deterioration.","authors":"Hongyuan Fu, Aijun Liu, Ming Yang, Zeyu Liu, Junwu Su","doi":"10.14503/THIJ-24-8523","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Mitral valvuloplasty is considered the best treatment for pediatric mitral valve regurgitation. The objective of this analysis was to identify risk factors for postoperative mitral valve regurgitation progression and evaluate valvuloplasty effectiveness.</p><p><strong>Methods: </strong>This retrospective, single-center study investigated the clinical efficacy of mitral valvuloplasty and identified factors that affect prognosis. Pediatric patients with moderate or severe mitral valve regurgitation who had undergone mitral valvuloplasty between September 2016 and August 2023 were included. Kaplan-Meier survival analysis was used to assess freedom from both mitral valve deterioration and cardiovascular death. Univariate and multivariate Cox regression analyses were performed to identify potential risk factors.</p><p><strong>Results: </strong>The study comprised 137 pediatric patients (mean age, 37.5 months [range, 2.4-167.6 months]) who had moderate (64/137 [46.7%]) or severe (73.137 [53.3%]) mitral valve regurgitation. At midterm follow-up (median, 55.3 months), mitral valve regurgitation had statistically significantly decreased compared with preoperative levels (<i>P</i> < .001, Wilcoxon signed-rank test); freedom from cardiovascular death was 97.5%, and freedom from worsening mitral valve regurgitation was 89.4%. Cox regression analysis identified body weight (<i>P</i> = .02), left ventricular end-diastolic diameter (<i>P</i> = .005), and left ventricular ejection fraction (<i>P</i> = .01) at 1 month and cardiopulmonary bypass time (<i>P</i> = .007) as independent risk factors for deterioration. Patients weighing 10 kg or more (<i>P</i> = .04) or with a ventricular septal defect 8 mm or larger (<i>P</i> = .04) had worse outcomes.</p><p><strong>Conclusion: </strong>Mitral valvuloplasty resulted in low mortality and positive long-term results in pediatric patients with mitral valve regurgitation. Early aggressive therapy is recommended to avoid late postoperative mitral valve deterioration.</p>","PeriodicalId":48680,"journal":{"name":"Texas Heart Institute Journal","volume":"52 2","pages":"e248523"},"PeriodicalIF":0.9000,"publicationDate":"2025-07-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12310506/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Texas Heart Institute Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14503/THIJ-24-8523","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Mitral valvuloplasty is considered the best treatment for pediatric mitral valve regurgitation. The objective of this analysis was to identify risk factors for postoperative mitral valve regurgitation progression and evaluate valvuloplasty effectiveness.
Methods: This retrospective, single-center study investigated the clinical efficacy of mitral valvuloplasty and identified factors that affect prognosis. Pediatric patients with moderate or severe mitral valve regurgitation who had undergone mitral valvuloplasty between September 2016 and August 2023 were included. Kaplan-Meier survival analysis was used to assess freedom from both mitral valve deterioration and cardiovascular death. Univariate and multivariate Cox regression analyses were performed to identify potential risk factors.
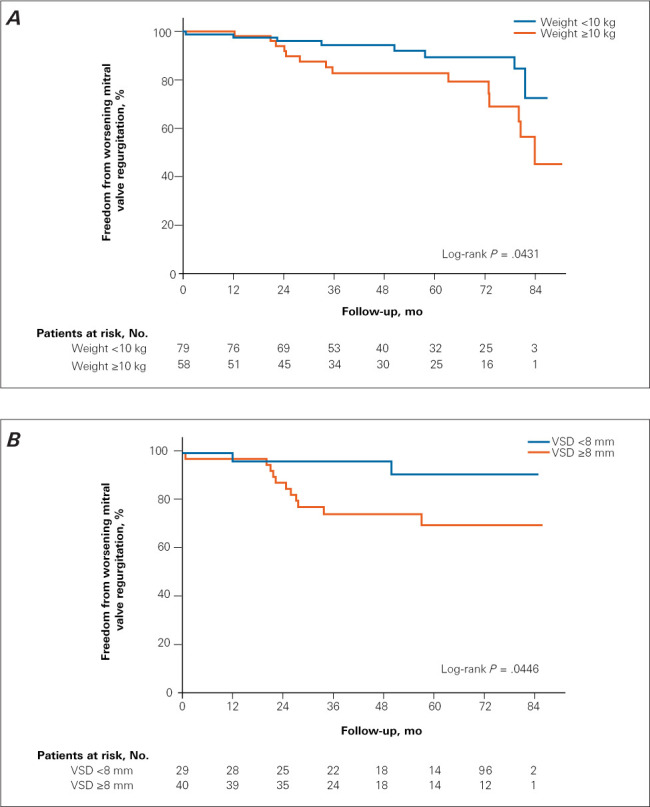
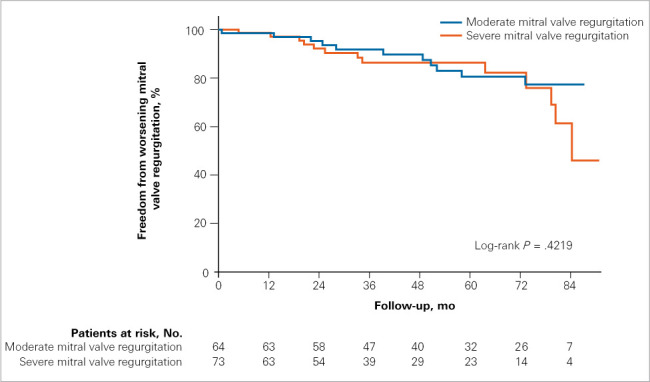
Results: The study comprised 137 pediatric patients (mean age, 37.5 months [range, 2.4-167.6 months]) who had moderate (64/137 [46.7%]) or severe (73.137 [53.3%]) mitral valve regurgitation. At midterm follow-up (median, 55.3 months), mitral valve regurgitation had statistically significantly decreased compared with preoperative levels (P < .001, Wilcoxon signed-rank test); freedom from cardiovascular death was 97.5%, and freedom from worsening mitral valve regurgitation was 89.4%. Cox regression analysis identified body weight (P = .02), left ventricular end-diastolic diameter (P = .005), and left ventricular ejection fraction (P = .01) at 1 month and cardiopulmonary bypass time (P = .007) as independent risk factors for deterioration. Patients weighing 10 kg or more (P = .04) or with a ventricular septal defect 8 mm or larger (P = .04) had worse outcomes.
Conclusion: Mitral valvuloplasty resulted in low mortality and positive long-term results in pediatric patients with mitral valve regurgitation. Early aggressive therapy is recommended to avoid late postoperative mitral valve deterioration.
期刊介绍:
For more than 45 years, the Texas Heart Institute Journal has been published by the Texas Heart Institute as part of its medical education program. Our bimonthly peer-reviewed journal enjoys a global audience of physicians, scientists, and healthcare professionals who are contributing to the prevention, diagnosis, and treatment of cardiovascular disease.
The Journal was printed under the name of Cardiovascular Diseases from 1974 through 1981 (ISSN 0093-3546). The name was changed to Texas Heart Institute Journal in 1982 and was printed through 2013 (ISSN 0730-2347). In 2014, the Journal moved to online-only publication. It is indexed by Index Medicus/MEDLINE and by other indexing and abstracting services worldwide. Our full archive is available at PubMed Central.
The Journal invites authors to submit these article types for review:
-Clinical Investigations-
Laboratory Investigations-
Reviews-
Techniques-
Coronary Anomalies-
History of Medicine-
Case Reports/Case Series (Submission Fee: $70.00 USD)-
Images in Cardiovascular Medicine (Submission Fee: $35.00 USD)-
Guest Editorials-
Peabody’s Corner-
Letters to the Editor

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


