Liver stiffness measurements in patients with metabolic dysfunction-associated steatotic liver disease: Updates on the method effectiveness and perspectives.
Olga Sukocheva, Tsai-Wing Ow, Damian Harding, Marc Le Mire, Edmund Tse
{"title":"Liver stiffness measurements in patients with metabolic dysfunction-associated steatotic liver disease: Updates on the method effectiveness and perspectives.","authors":"Olga Sukocheva, Tsai-Wing Ow, Damian Harding, Marc Le Mire, Edmund Tse","doi":"10.4254/wjh.v17.i7.106675","DOIUrl":null,"url":null,"abstract":"<p><p>Metabolic dysfunction-associated steatotic liver disease (MASLD) is the most widespread chronic liver disease signified by serious life-threatening conditions. The prevalence of MASLD increases along the growing prevalence in obesity and metabolic syndrome. To minimize costs and complications, non-invasive diagnostic tools, including transient elastography (TE), were introduced for assessment of MASLD. TE measures liver stiffness (LS), a clinical marker for the diagnosis of liver fibrosis and cirrhosis. LS measurements are based on ultrasound wave imaging and quantification. Vibration-controlled TE, including FibroScan<sup>®</sup>, is commonly used TE methods which can accurately identify the degree of liver fibrosis and cirrhosis progression. TE was reported to predict the progression towards hepatocellular carcinoma, portal hypertension, and varices. However, the accuracy of LS diagnostics alone in patients with MASLD remains controversial. TE measurements have several limitations, including inadequate precision due to focal liver lesions, cholestasis, inflammation, and other pathological and anatomical factors which can lead to the stiffness variability. Overestimations of TE readings were reported in obese patients with body mass index (BMI) over 30 kg/m<sup>2</sup>, and older patients with ascites, diabetes, or hypertension. Not all MASLD patients have high BMI. The prevalence of obesity among MASLD patients varies worldwide, indicating the urgent need for comprehensive diagnostic tools. In patients with MASLD, improved diagnostic accuracy has been demonstrated by combining LS measurements with other blood test-based scores and simple clinical parameters (agile scores based on age, sex, platelet count, aminotransferases, and diabetes). This study reviews the limitations of TE-based diagnostics and discusses the combined scoring algorithm. In conclusion, the sequence of LS measurements along assessment of other important clinical markers is an effective, low-cost, reliable tool to identify and monitor fibrosis progression in MASLD.</p>","PeriodicalId":23687,"journal":{"name":"World Journal of Hepatology","volume":"17 7","pages":"106675"},"PeriodicalIF":2.5000,"publicationDate":"2025-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12308552/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Hepatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4254/wjh.v17.i7.106675","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
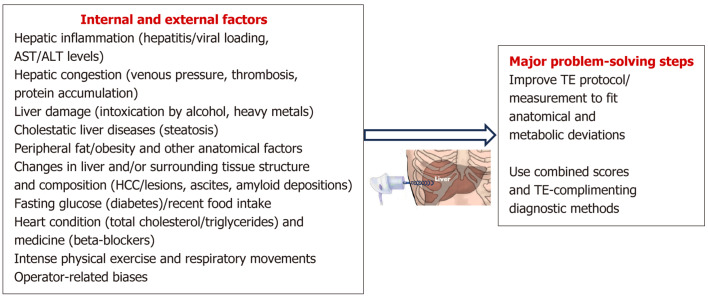
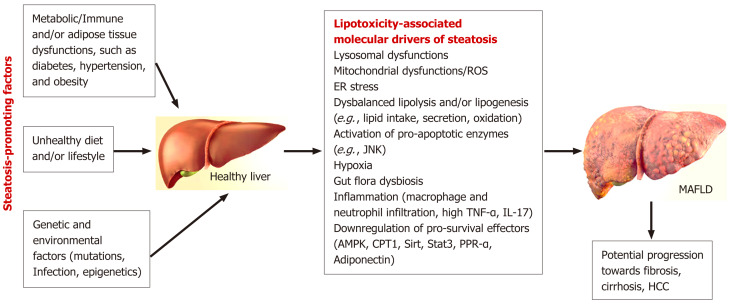
Metabolic dysfunction-associated steatotic liver disease (MASLD) is the most widespread chronic liver disease signified by serious life-threatening conditions. The prevalence of MASLD increases along the growing prevalence in obesity and metabolic syndrome. To minimize costs and complications, non-invasive diagnostic tools, including transient elastography (TE), were introduced for assessment of MASLD. TE measures liver stiffness (LS), a clinical marker for the diagnosis of liver fibrosis and cirrhosis. LS measurements are based on ultrasound wave imaging and quantification. Vibration-controlled TE, including FibroScan®, is commonly used TE methods which can accurately identify the degree of liver fibrosis and cirrhosis progression. TE was reported to predict the progression towards hepatocellular carcinoma, portal hypertension, and varices. However, the accuracy of LS diagnostics alone in patients with MASLD remains controversial. TE measurements have several limitations, including inadequate precision due to focal liver lesions, cholestasis, inflammation, and other pathological and anatomical factors which can lead to the stiffness variability. Overestimations of TE readings were reported in obese patients with body mass index (BMI) over 30 kg/m2, and older patients with ascites, diabetes, or hypertension. Not all MASLD patients have high BMI. The prevalence of obesity among MASLD patients varies worldwide, indicating the urgent need for comprehensive diagnostic tools. In patients with MASLD, improved diagnostic accuracy has been demonstrated by combining LS measurements with other blood test-based scores and simple clinical parameters (agile scores based on age, sex, platelet count, aminotransferases, and diabetes). This study reviews the limitations of TE-based diagnostics and discusses the combined scoring algorithm. In conclusion, the sequence of LS measurements along assessment of other important clinical markers is an effective, low-cost, reliable tool to identify and monitor fibrosis progression in MASLD.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


