{"title":"A prognostic score based on early recurrence-related factors for hepatocellular carcinoma patients with microvascular invasion after hepatectomy.","authors":"Hongyu Li, Junyi Shen, Tianfu Wen","doi":"10.1007/s00423-025-03823-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>We aimed to construct a simple risk score to stratify individuals with distinguished prognosis for HCC patients with microvascular invasion (MVI).</p><p><strong>Methods: </strong>265 qualified patients were retrospectively analyzed. A prognostic score was constructed using predictors associated with early recurrence (ER). Based on the HR value, AFP > 400 ng/ml and hepatitis B viral e antigen (HBeAg) positivity were assigned as 1 point, satellite nodule was assigned 2 points. There were five subgroups (score 0/1/2/3/4). Due to similar RFS in score 2/3/4 subgroups, we merged these into a single cohort (group C), while maintaining score 0 as group A and score 1 as group B.</p><p><strong>Results: </strong>MVI (+) HCC patients who developed ER had dramatically decreased overall survival (OS) compared with those who did not(P < 0.001). Based on the result of multivariable analysis, MVI (+) HCC patients with satellite nodules, positive HBeAg or serum alpha-fetoprotein above 400ng/ml were more likely to developed ER. The 3-year recurrence free survival rates for the group A, group B and group C were 42.7%, 26.4% and 9.3%, respectively. The 3-year OS rates for group A, group B and group C were 65.4%, 48.7% and 26.9%, respectively (p < 0.001). A higher score was correlated with significantly worse prognosis (p < 0.001). Furthermore, the prognostic score distinguished the prognosis of MVI (+) HCC patients independently of liver cirrhosis (p < 0.001).</p><p><strong>Conclusions: </strong>The prognostic score consisted of ER-related factors effectively predict prognosis for MVI (+) HCC patients after hepatectomy.</p>","PeriodicalId":17983,"journal":{"name":"Langenbeck's Archives of Surgery","volume":"410 1","pages":"237"},"PeriodicalIF":1.8000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12316790/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Langenbeck's Archives of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00423-025-03823-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: We aimed to construct a simple risk score to stratify individuals with distinguished prognosis for HCC patients with microvascular invasion (MVI).
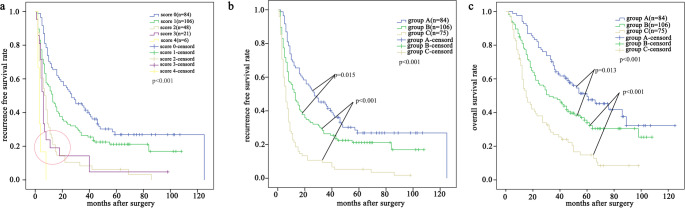
Methods: 265 qualified patients were retrospectively analyzed. A prognostic score was constructed using predictors associated with early recurrence (ER). Based on the HR value, AFP > 400 ng/ml and hepatitis B viral e antigen (HBeAg) positivity were assigned as 1 point, satellite nodule was assigned 2 points. There were five subgroups (score 0/1/2/3/4). Due to similar RFS in score 2/3/4 subgroups, we merged these into a single cohort (group C), while maintaining score 0 as group A and score 1 as group B.
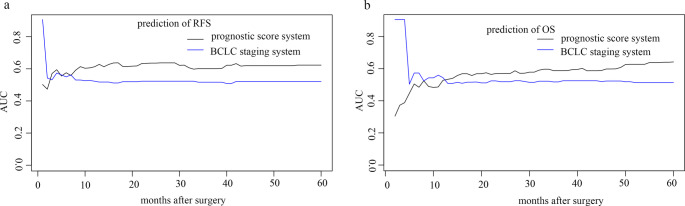
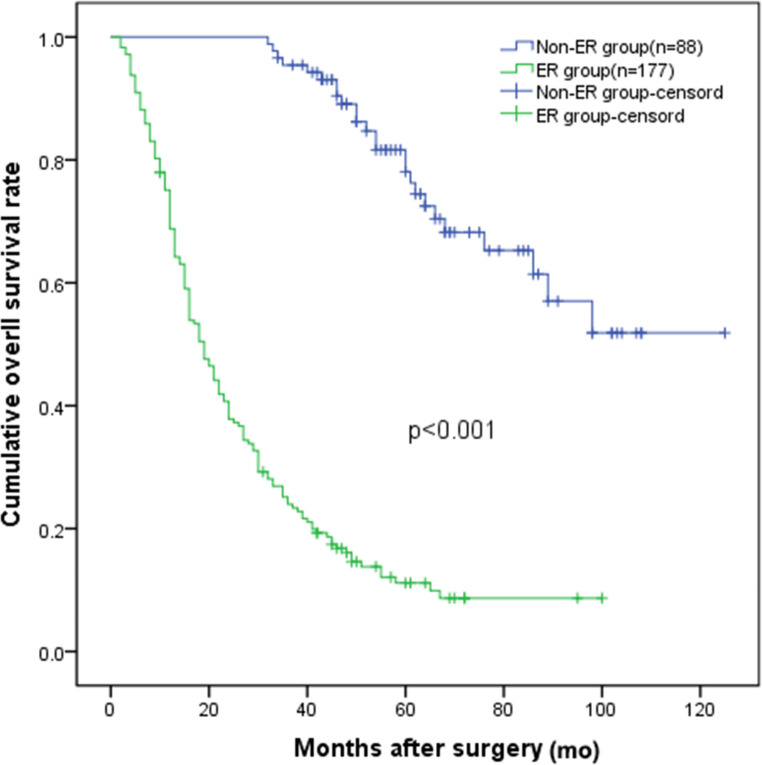
Results: MVI (+) HCC patients who developed ER had dramatically decreased overall survival (OS) compared with those who did not(P < 0.001). Based on the result of multivariable analysis, MVI (+) HCC patients with satellite nodules, positive HBeAg or serum alpha-fetoprotein above 400ng/ml were more likely to developed ER. The 3-year recurrence free survival rates for the group A, group B and group C were 42.7%, 26.4% and 9.3%, respectively. The 3-year OS rates for group A, group B and group C were 65.4%, 48.7% and 26.9%, respectively (p < 0.001). A higher score was correlated with significantly worse prognosis (p < 0.001). Furthermore, the prognostic score distinguished the prognosis of MVI (+) HCC patients independently of liver cirrhosis (p < 0.001).
Conclusions: The prognostic score consisted of ER-related factors effectively predict prognosis for MVI (+) HCC patients after hepatectomy.
期刊介绍:
Langenbeck''s Archives of Surgery aims to publish the best results in the field of clinical surgery and basic surgical research. The main focus is on providing the highest level of clinical research and clinically relevant basic research. The journal, published exclusively in English, will provide an international discussion forum for the controlled results of clinical surgery. The majority of published contributions will be original articles reporting on clinical data from general and visceral surgery, while endocrine surgery will also be covered. Papers on basic surgical principles from the fields of traumatology, vascular and thoracic surgery are also welcome. Evidence-based medicine is an important criterion for the acceptance of papers.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


