Stein Arne Rimehaug, Rikke Helene Moe, Hanne Dagfinrud, Felix Fischer, Thomas Johansen, Ingvild Kjeken, Mari Klokkerud, Hanne Ludt Fossmo, Anne Dorte Lyken, Tarja Rajalahti Kvalheim, Silje Soldal, Anne-Lene Sand-Svartrud
{"title":"Measurement properties of the PROMIS-29 profile v2.1 in a Norwegian rehabilitation context.","authors":"Stein Arne Rimehaug, Rikke Helene Moe, Hanne Dagfinrud, Felix Fischer, Thomas Johansen, Ingvild Kjeken, Mari Klokkerud, Hanne Ludt Fossmo, Anne Dorte Lyken, Tarja Rajalahti Kvalheim, Silje Soldal, Anne-Lene Sand-Svartrud","doi":"10.1186/s41687-025-00929-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Psychometric properties of the Patient-Reported Outcomes Measurement Information System<sup>®</sup> Profile 29 (PROMIS-29) Norwegian version has previously been examined in a general population. This multicenter study aimed to examine the internal consistency, construct validity, responsiveness, score distribution and floor/ceiling effects of PROMIS-29 v2.1 in a Norwegian rehabilitation context.</p><p><strong>Methods: </strong>Patients receiving rehabilitation services participating in a longitudinal cohort study answered PROMIS-29 at baseline and at 3-month follow-up. Internal consistency was assessed by Cronbach's alpha and McDonald's omega. Construct validity was examined through hypothesis testing, using EQ-5D-5L as comparator measure. Hypotheses for correlations of change scores for both questionnaires were tested as an expression of responsiveness. Score distribution and floor/ceiling effects were examined with histograms and descriptive statistics.</p><p><strong>Results: </strong>A total of 828 patients with a mean age of 54.3 years were included for analysis. The internal consistency for each PROMIS-29 domain was confirmed, with alpha and omega values exceeding the threshold of ≥ 0.70. Regarding correlations between PROMIS-29 and EQ-5D-5L, 34 out of 40 hypotheses were confirmed for construct validity and 19 out of 24 for responsiveness, both meeting our a priori criterion of ≥ 75% confirmed hypotheses. There was no floor effect of any PROMIS-29 domain in our sample, and ceiling effect only for anxiety and depression domain scores. Still, this confirmed the applicability of PROMIS-29 in a rehabilitation context.</p><p><strong>Conclusion: </strong>The Norwegian PROMIS-29 has sufficient internal consistency, construct validity and responsiveness for use as an outcome measure for health status and health-related quality of life in rehabilitation.</p><p><strong>Trial registration number: </strong>ClinicalTrials.gov NCT03764982 RehabNytte study, registered 2018-12-04.</p>","PeriodicalId":36660,"journal":{"name":"Journal of Patient-Reported Outcomes","volume":"9 1","pages":"98"},"PeriodicalIF":2.9000,"publicationDate":"2025-07-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12314140/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Patient-Reported Outcomes","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41687-025-00929-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Psychometric properties of the Patient-Reported Outcomes Measurement Information System® Profile 29 (PROMIS-29) Norwegian version has previously been examined in a general population. This multicenter study aimed to examine the internal consistency, construct validity, responsiveness, score distribution and floor/ceiling effects of PROMIS-29 v2.1 in a Norwegian rehabilitation context.
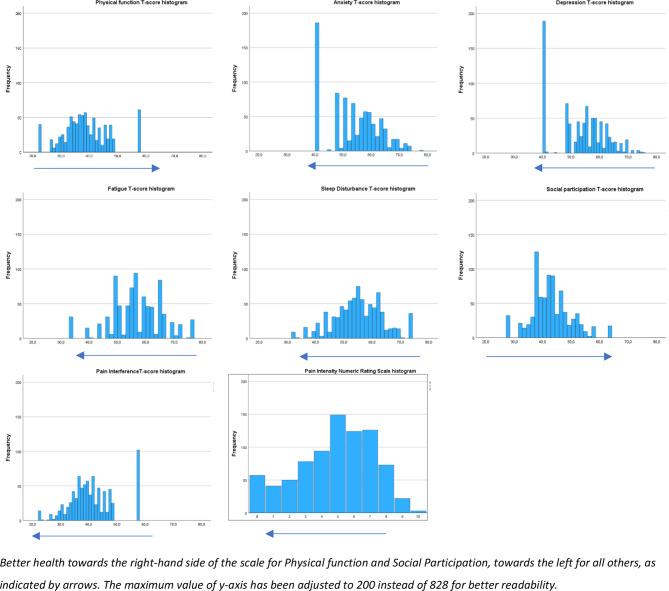
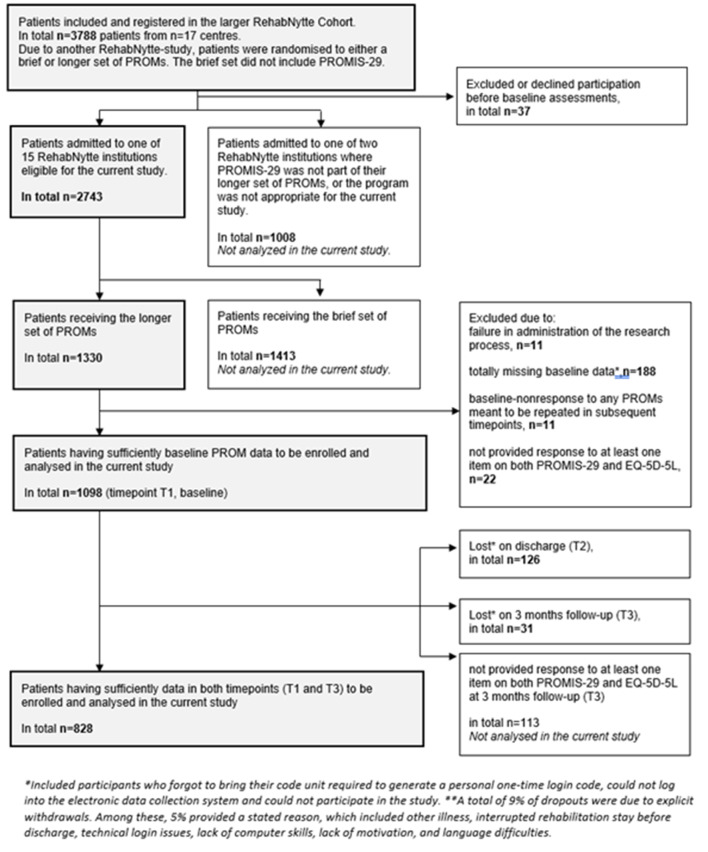
Methods: Patients receiving rehabilitation services participating in a longitudinal cohort study answered PROMIS-29 at baseline and at 3-month follow-up. Internal consistency was assessed by Cronbach's alpha and McDonald's omega. Construct validity was examined through hypothesis testing, using EQ-5D-5L as comparator measure. Hypotheses for correlations of change scores for both questionnaires were tested as an expression of responsiveness. Score distribution and floor/ceiling effects were examined with histograms and descriptive statistics.
Results: A total of 828 patients with a mean age of 54.3 years were included for analysis. The internal consistency for each PROMIS-29 domain was confirmed, with alpha and omega values exceeding the threshold of ≥ 0.70. Regarding correlations between PROMIS-29 and EQ-5D-5L, 34 out of 40 hypotheses were confirmed for construct validity and 19 out of 24 for responsiveness, both meeting our a priori criterion of ≥ 75% confirmed hypotheses. There was no floor effect of any PROMIS-29 domain in our sample, and ceiling effect only for anxiety and depression domain scores. Still, this confirmed the applicability of PROMIS-29 in a rehabilitation context.
Conclusion: The Norwegian PROMIS-29 has sufficient internal consistency, construct validity and responsiveness for use as an outcome measure for health status and health-related quality of life in rehabilitation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


