Single-Entry Selective Trunk Block (S-SeTB): An Innovative Approach to Complete Upper Extremity Anesthesia in Weapon-Wounded Patients in Low-Resource Settings.
{"title":"Single-Entry Selective Trunk Block (S-SeTB): An Innovative Approach to Complete Upper Extremity Anesthesia in Weapon-Wounded Patients in Low-Resource Settings.","authors":"Majaliwa Shabani, Sophie Crespo, Xavier Raingeval","doi":"10.2147/LRA.S524347","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Regional anesthesia for upper extremity surgery in weapon-wounded patients is challenging, particularly in low-resource settings. Existing techniques often require multiple needle entries and ultrasound probe repositioning, increasing complexity and risk. There is a need for a simpler, effective technique providing complete anesthesia from the shoulder to the hand.</p><p><strong>Methods: </strong>We developed a novel ultrasound-guided regional anesthesia technique-the Single-entry Selective Trunk Block (S-SeTB)-which targets the superior trunk (ST), middle trunk (MT), and C8 ventral ramus (C8VR) with local anesthetic diffusion to the inferior trunk (IT). The procedure uses one skin entry point to deliver three injections and is combined with a superficial cervical plexus (SCP) block using the same entry and ultrasound plane. Over 600 procedures were performed in field hospitals operated by the International Committee of the Red Cross, with observations documented.</p><p><strong>Results: </strong>The S-SeTB consistently achieved full anesthesia of the upper extremity, including the shoulder and clavicle, without the need for conversion to general anesthesia. The technique was well tolerated and effective in complex trauma cases. No major complications were reported. Compared to conventional selective trunk blocks or hybrid brachial plexus approaches, the S-SeTB required lower anesthetic volumes (20-25 mL) and demonstrated reduced procedural complexity and risks (eg, pneumothorax, vascular puncture).</p><p><strong>Conclusion: </strong>The S-SeTB, combined with SCP and intercostobrachial nerve blocks, offers a reliable, resource-efficient, and safer alternative to traditional brachial plexus block techniques. It is particularly well-suited for austere environments where anesthesia resources and safety margins are limited. Further prospective studies are ongoing to evaluate block dynamics and confirm efficacy.</p>","PeriodicalId":18203,"journal":{"name":"Local and Regional Anesthesia","volume":"18 ","pages":"45-55"},"PeriodicalIF":1.9000,"publicationDate":"2025-07-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12309568/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Local and Regional Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LRA.S524347","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Regional anesthesia for upper extremity surgery in weapon-wounded patients is challenging, particularly in low-resource settings. Existing techniques often require multiple needle entries and ultrasound probe repositioning, increasing complexity and risk. There is a need for a simpler, effective technique providing complete anesthesia from the shoulder to the hand.
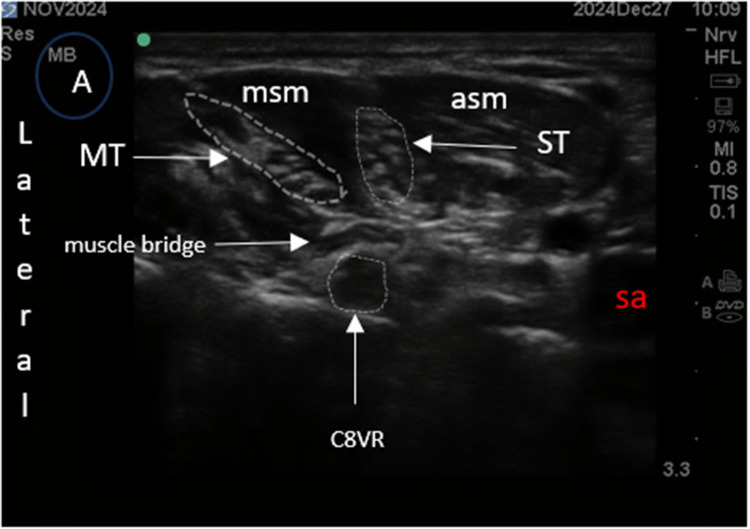
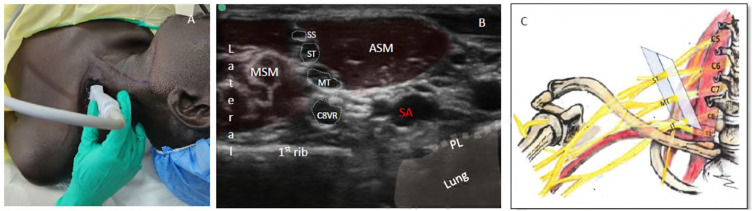
Methods: We developed a novel ultrasound-guided regional anesthesia technique-the Single-entry Selective Trunk Block (S-SeTB)-which targets the superior trunk (ST), middle trunk (MT), and C8 ventral ramus (C8VR) with local anesthetic diffusion to the inferior trunk (IT). The procedure uses one skin entry point to deliver three injections and is combined with a superficial cervical plexus (SCP) block using the same entry and ultrasound plane. Over 600 procedures were performed in field hospitals operated by the International Committee of the Red Cross, with observations documented.
Results: The S-SeTB consistently achieved full anesthesia of the upper extremity, including the shoulder and clavicle, without the need for conversion to general anesthesia. The technique was well tolerated and effective in complex trauma cases. No major complications were reported. Compared to conventional selective trunk blocks or hybrid brachial plexus approaches, the S-SeTB required lower anesthetic volumes (20-25 mL) and demonstrated reduced procedural complexity and risks (eg, pneumothorax, vascular puncture).
Conclusion: The S-SeTB, combined with SCP and intercostobrachial nerve blocks, offers a reliable, resource-efficient, and safer alternative to traditional brachial plexus block techniques. It is particularly well-suited for austere environments where anesthesia resources and safety margins are limited. Further prospective studies are ongoing to evaluate block dynamics and confirm efficacy.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


