{"title":"Voriconazole-induced liver injury: incidence patterns and risk factors in a retrospective cohort.","authors":"Yan Lou, Yu Wang, Jing Liu, Yu-Jing Wang, Jiaqi Wang, Shuang Ma, Zong-Ming Yang, Jing-Song Li, Yun-Qing Qiu","doi":"10.1128/aac.00487-25","DOIUrl":null,"url":null,"abstract":"<p><p>Voriconazole, a first-line therapy for invasive aspergillosis, carries hepatotoxicity risks lacking comprehensive epidemiological characterization. Current evidence is limited by heterogeneity in diagnostic criteria (e.g., varying thresholds for liver function abnormalities across studies), insufficient sample sizes, and inadequate adjustment for comorbidities, which compromises risk assessment accuracy. This study aims to systematically characterize the epidemiological profile of voriconazole-induced liver injury and identify modifiable independent risk factors. We analyzed 7,659 voriconazole-treated adults (2007-2020) from the First Affiliated Hospital of Zhejiang University to determine incidence and injury subtypes. Univariable and multivariable logistic regression identified risk factors, with model performance evaluated by ROC (receiver-operating characteristic) analysis; sensitivity analyses addressed potential confounders. In our results, voriconazole-induced liver injury occurred in 11.32% of patients, predominantly manifesting as hepatocellular (5.01%, 279/630), cholestatic (5.19%, 289/630), and mixed-pattern injuries (1.11%, 62/630). Key modifiable risk factors included intravenous administration (odds ratio [OR] = 1.88, 95% confidence interval [CI]: 1.43-2.46). Non-modifiable predictors comprised baseline elevated urea (OR = 1.47, 95% CI: 1.08-2.02), elevated triglycerides (TG) (cholestatic injury: OR = 1.47, 95% CI: 1.08-2.02), elevated C-reactive protein (CRP) (cholestatic injury: OR = 1.47, 95% CI: 1.08-2.02), pre-existing liver disease (liver cirrhosis, OR = 2.16, 95% CI: 1.58-2.96), diabetes (OR = 2.19, 95% CI: 1.70-2.80), and transplant status (hematopoietic stem cell transplantation, OR = 2.93, 95% CI: 1.85-4.65). Using this clinically substantial cohort (<i>n</i>=7,659), we proposed a risk-stratification framework incorporating administration route optimization and comorbidity-specific monitoring, supporting personalized risk-benefit analysis in antifungal therapy.</p>","PeriodicalId":8152,"journal":{"name":"Antimicrobial Agents and Chemotherapy","volume":" ","pages":"e0048725"},"PeriodicalIF":4.5000,"publicationDate":"2025-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406674/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Antimicrobial Agents and Chemotherapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1128/aac.00487-25","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/31 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"MICROBIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
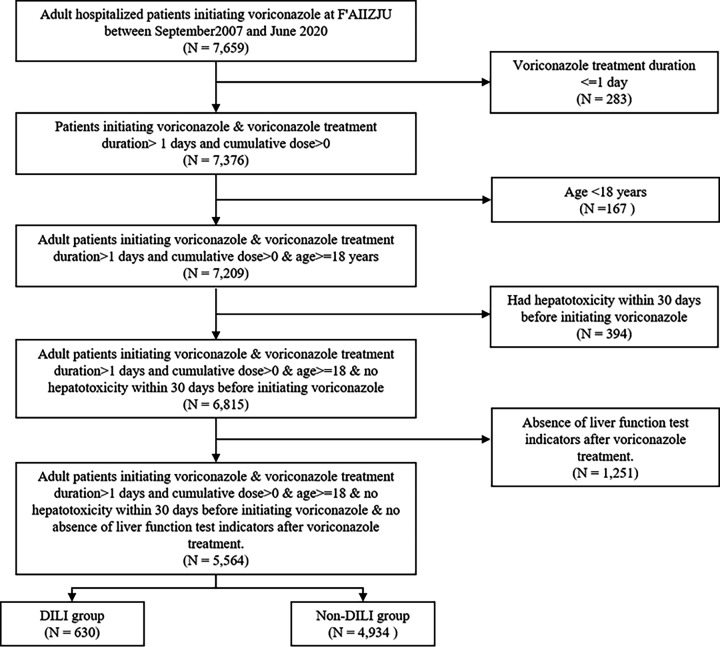
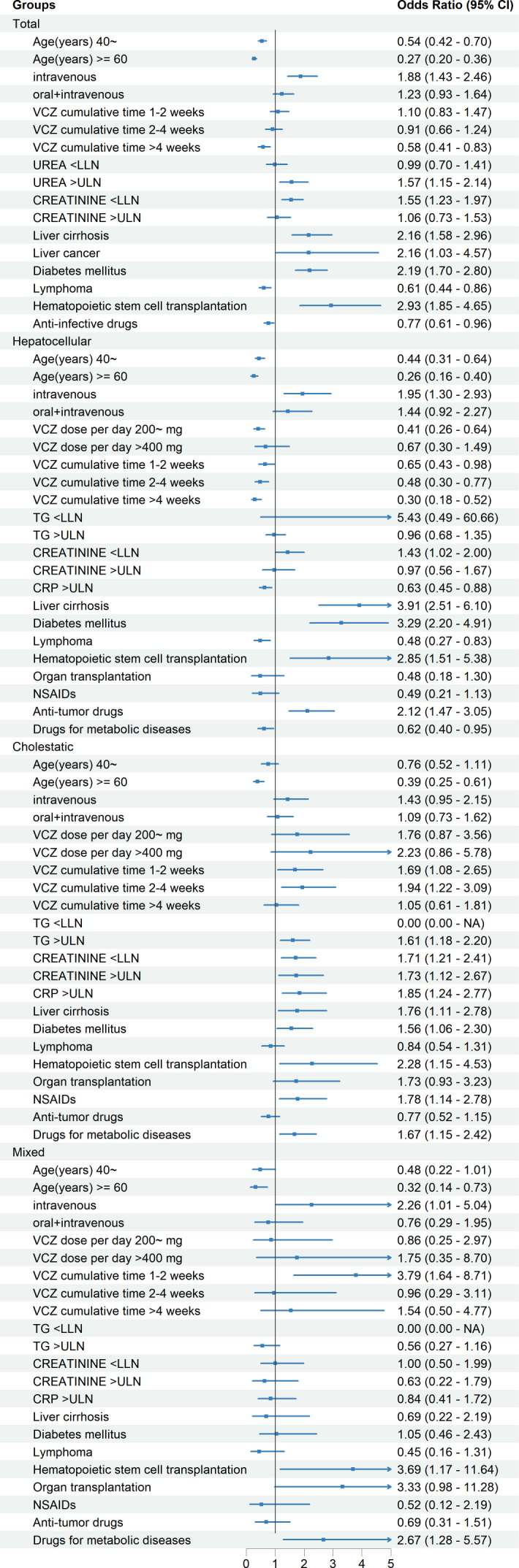
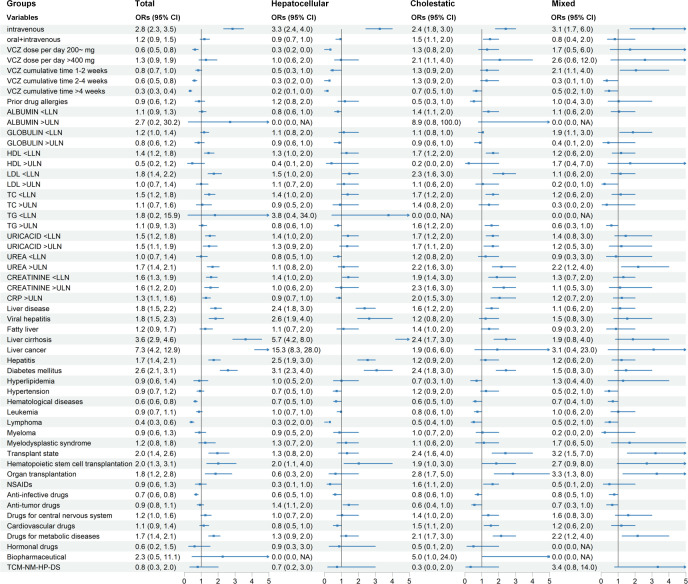
Voriconazole, a first-line therapy for invasive aspergillosis, carries hepatotoxicity risks lacking comprehensive epidemiological characterization. Current evidence is limited by heterogeneity in diagnostic criteria (e.g., varying thresholds for liver function abnormalities across studies), insufficient sample sizes, and inadequate adjustment for comorbidities, which compromises risk assessment accuracy. This study aims to systematically characterize the epidemiological profile of voriconazole-induced liver injury and identify modifiable independent risk factors. We analyzed 7,659 voriconazole-treated adults (2007-2020) from the First Affiliated Hospital of Zhejiang University to determine incidence and injury subtypes. Univariable and multivariable logistic regression identified risk factors, with model performance evaluated by ROC (receiver-operating characteristic) analysis; sensitivity analyses addressed potential confounders. In our results, voriconazole-induced liver injury occurred in 11.32% of patients, predominantly manifesting as hepatocellular (5.01%, 279/630), cholestatic (5.19%, 289/630), and mixed-pattern injuries (1.11%, 62/630). Key modifiable risk factors included intravenous administration (odds ratio [OR] = 1.88, 95% confidence interval [CI]: 1.43-2.46). Non-modifiable predictors comprised baseline elevated urea (OR = 1.47, 95% CI: 1.08-2.02), elevated triglycerides (TG) (cholestatic injury: OR = 1.47, 95% CI: 1.08-2.02), elevated C-reactive protein (CRP) (cholestatic injury: OR = 1.47, 95% CI: 1.08-2.02), pre-existing liver disease (liver cirrhosis, OR = 2.16, 95% CI: 1.58-2.96), diabetes (OR = 2.19, 95% CI: 1.70-2.80), and transplant status (hematopoietic stem cell transplantation, OR = 2.93, 95% CI: 1.85-4.65). Using this clinically substantial cohort (n=7,659), we proposed a risk-stratification framework incorporating administration route optimization and comorbidity-specific monitoring, supporting personalized risk-benefit analysis in antifungal therapy.
期刊介绍:
Antimicrobial Agents and Chemotherapy (AAC) features interdisciplinary studies that build our understanding of the underlying mechanisms and therapeutic applications of antimicrobial and antiparasitic agents and chemotherapy.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


