Melanie J Woodfield, Sarah Fortune, Tania Cargo, Sally Merry, Sarah E Hetrick
{"title":"Re-Implementation of Parent-Child Interaction Therapy (PCIT) in the Community: Findings From a Pilot Randomized Controlled Trial.","authors":"Melanie J Woodfield, Sarah Fortune, Tania Cargo, Sally Merry, Sarah E Hetrick","doi":"10.1177/26334895251363418","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study explored the feasibility, acceptability, and Māori cultural responsivity of study methods and components of an intervention to support clinicians to resume implementation of Parent-Child Interaction Therapy (PCIT), an evidence-based treatment for disruptive behavior in young children.</p><p><strong>Method: </strong>This pragmatic, parallel-arm, randomized, controlled pilot trial ran for a 6-month period and included PCIT-trained clinicians who were not delivering, or only rarely using PCIT in their work. Re-implementation strategies were systematically developed and theory-driven and included a mobile co-worker, a portable time-out space, audio-visual equipment, weekly consultation groups, and 2-day targeted PCIT refresher training.</p><p><strong>Results: </strong>Pre-specified progression criteria included enrolling 20 clinicians, a maximum of 20% attrition, and a monthly survey response rate of at least 80%. Fourteen clinicians enrolled in the trial, there was no attrition, and an 89.8% average survey response rate was achieved. Secondary outcomes included clinician ratings of the usefulness and acceptability of intervention components. The time-out cubicle was considered relatively less useful and acceptable, while the refresher training and manuals were preferred. Study methods and intervention components were considered acceptable by the small proportion of Māori participants. Clinician self-reported Capability, Opportunity, and Motivation to implement PCIT fluctuated monthly across both groups. Pre-/post-changes in each domain within the Theoretical Domains Framework generally showed similar improvement from baseline to follow-up in both groups. There was no observable difference in PCIT adoption in either group.</p><p><strong>Conclusion: </strong>To the best of our knowledge, this is the first study to pragmatically attempt to re-implement a parent training intervention in a community setting, several years after clinicians' initial training in the approach (here, an average of 5.36 years). Low attrition and high survey response rates highlighted the feasibility of the data collection methodology. Important opportunities to improve the design of an adequately powered definitive trial are highlighted to minimize future resource waste.</p>","PeriodicalId":73354,"journal":{"name":"Implementation research and practice","volume":"6 ","pages":"26334895251363418"},"PeriodicalIF":2.6000,"publicationDate":"2025-07-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12304612/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334895251363418","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This study explored the feasibility, acceptability, and Māori cultural responsivity of study methods and components of an intervention to support clinicians to resume implementation of Parent-Child Interaction Therapy (PCIT), an evidence-based treatment for disruptive behavior in young children.
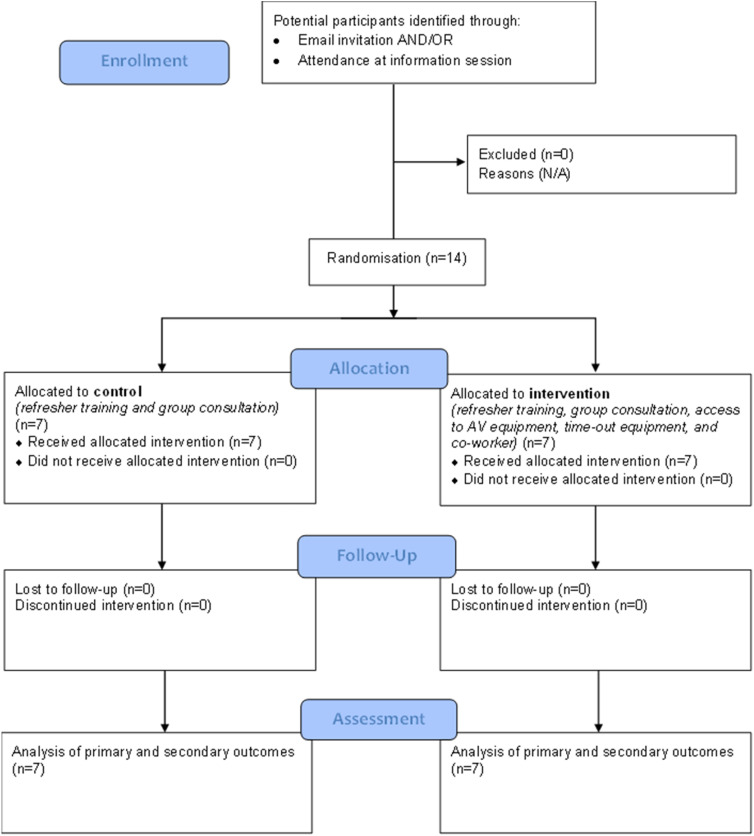
Method: This pragmatic, parallel-arm, randomized, controlled pilot trial ran for a 6-month period and included PCIT-trained clinicians who were not delivering, or only rarely using PCIT in their work. Re-implementation strategies were systematically developed and theory-driven and included a mobile co-worker, a portable time-out space, audio-visual equipment, weekly consultation groups, and 2-day targeted PCIT refresher training.
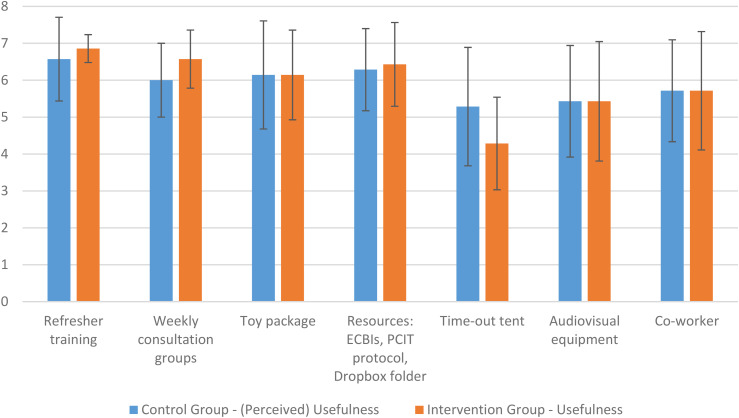
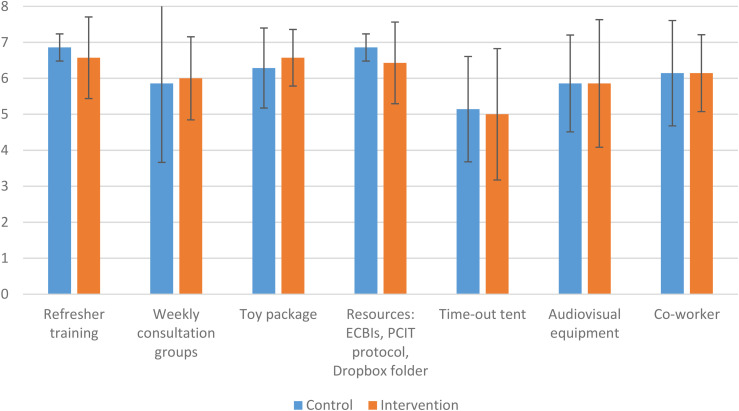
Results: Pre-specified progression criteria included enrolling 20 clinicians, a maximum of 20% attrition, and a monthly survey response rate of at least 80%. Fourteen clinicians enrolled in the trial, there was no attrition, and an 89.8% average survey response rate was achieved. Secondary outcomes included clinician ratings of the usefulness and acceptability of intervention components. The time-out cubicle was considered relatively less useful and acceptable, while the refresher training and manuals were preferred. Study methods and intervention components were considered acceptable by the small proportion of Māori participants. Clinician self-reported Capability, Opportunity, and Motivation to implement PCIT fluctuated monthly across both groups. Pre-/post-changes in each domain within the Theoretical Domains Framework generally showed similar improvement from baseline to follow-up in both groups. There was no observable difference in PCIT adoption in either group.
Conclusion: To the best of our knowledge, this is the first study to pragmatically attempt to re-implement a parent training intervention in a community setting, several years after clinicians' initial training in the approach (here, an average of 5.36 years). Low attrition and high survey response rates highlighted the feasibility of the data collection methodology. Important opportunities to improve the design of an adequately powered definitive trial are highlighted to minimize future resource waste.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


