{"title":"Racial Disparities in Quality of Dental Care Among Publicly Insured Children.","authors":"Sung Eun Choi, Rindala Fayyad, Sharon-Lise Normand","doi":"10.1097/MLR.0000000000002184","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Reducing oral health disparities requires identifying subgroups experiencing gaps in quality of dental care and the sizes of those gaps. This study measured magnitudes and trends of racial/ethnic disparities in overall quality of dental care and examined factors contributing to the disparities.</p><p><strong>Methods: </strong>This retrospective cohort study used claims data from beneficiaries under age 21 enrolled in Medicaid and Children's Health Insurance Program in 6 states during 2015-2019. A standardized composite score of dental care quality was derived from 6 dental quality measures using Item Response Theory. Robust mixed-effect regression estimated the magnitudes and trends of quality disparities, adjusting for person-level covariates. A Blinder-Oaxaca decomposition quantified the relative contributions of the social and structural factors in the estimated racial/ethnic disparities.</p><p><strong>Results: </strong>Among 3.4 million beneficiaries, compared with White counterparts, Black children had lower baseline quality scores in 2 states and experienced decreases in quality in most states. Children of other race had lower baseline quality scores in 4 states with the largest gap of -0.16 (95% CI: -0.18,-0.15) and experienced decreases in quality in 3 states. Hispanic children had the higher baseline quality scores in all states with the largest gap of 0.34 (95% CI: 0.34,0.35) and experienced increases in quality in 4 states. Decomposition analysis indicated that structural factors, such as residential segregation, place of dental care, and dentist supply, explained portions of the quality gaps.</p><p><strong>Conclusion: </strong>Dental care quality was lower among Black and children of other race and higher among Hispanic and Asian children relative to their White counterparts. Tailored quality improvement efforts and refinements in Medicaid policy would be encouraged to reduce disparities in dental care and oral health.</p>","PeriodicalId":18364,"journal":{"name":"Medical Care","volume":" ","pages":"646-655"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12327499/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/MLR.0000000000002184","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/7 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Reducing oral health disparities requires identifying subgroups experiencing gaps in quality of dental care and the sizes of those gaps. This study measured magnitudes and trends of racial/ethnic disparities in overall quality of dental care and examined factors contributing to the disparities.
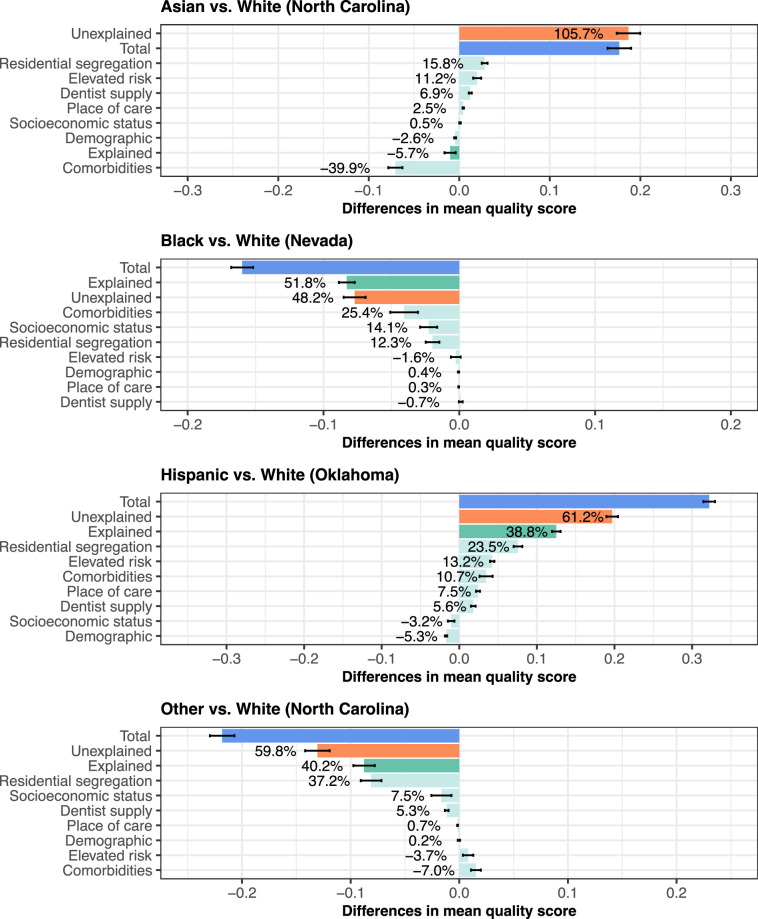
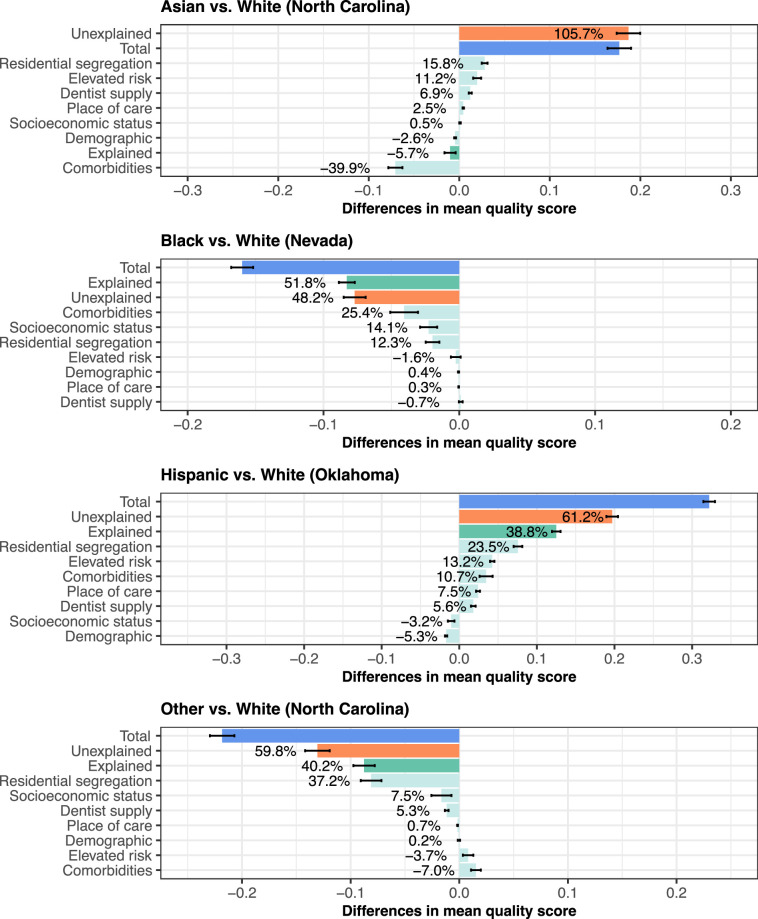
Methods: This retrospective cohort study used claims data from beneficiaries under age 21 enrolled in Medicaid and Children's Health Insurance Program in 6 states during 2015-2019. A standardized composite score of dental care quality was derived from 6 dental quality measures using Item Response Theory. Robust mixed-effect regression estimated the magnitudes and trends of quality disparities, adjusting for person-level covariates. A Blinder-Oaxaca decomposition quantified the relative contributions of the social and structural factors in the estimated racial/ethnic disparities.
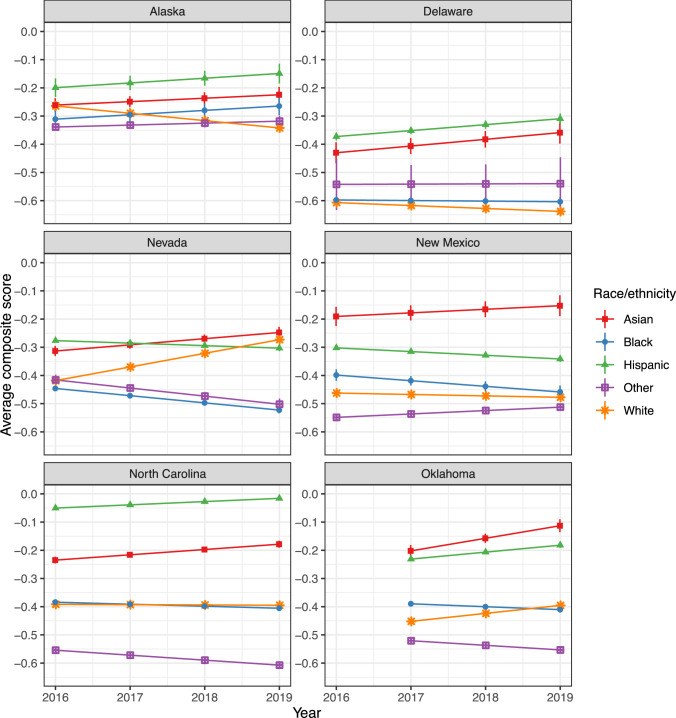
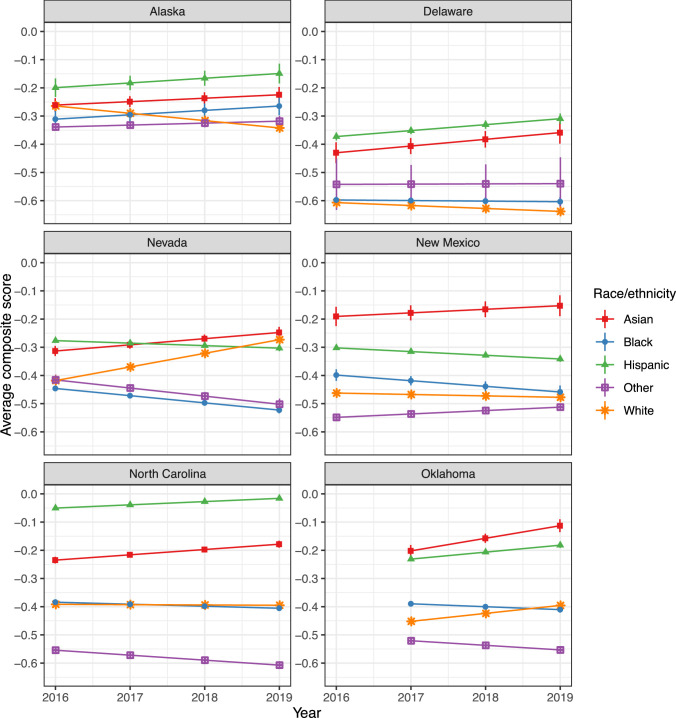
Results: Among 3.4 million beneficiaries, compared with White counterparts, Black children had lower baseline quality scores in 2 states and experienced decreases in quality in most states. Children of other race had lower baseline quality scores in 4 states with the largest gap of -0.16 (95% CI: -0.18,-0.15) and experienced decreases in quality in 3 states. Hispanic children had the higher baseline quality scores in all states with the largest gap of 0.34 (95% CI: 0.34,0.35) and experienced increases in quality in 4 states. Decomposition analysis indicated that structural factors, such as residential segregation, place of dental care, and dentist supply, explained portions of the quality gaps.
Conclusion: Dental care quality was lower among Black and children of other race and higher among Hispanic and Asian children relative to their White counterparts. Tailored quality improvement efforts and refinements in Medicaid policy would be encouraged to reduce disparities in dental care and oral health.
期刊介绍:
Rated as one of the top ten journals in healthcare administration, Medical Care is devoted to all aspects of the administration and delivery of healthcare. This scholarly journal publishes original, peer-reviewed papers documenting the most current developments in the rapidly changing field of healthcare. This timely journal reports on the findings of original investigations into issues related to the research, planning, organization, financing, provision, and evaluation of health services.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


