Influence of intercostal nerve block preemptive analgesia and incisional infiltration anesthesia on postoperative pain in patients undergoing laparoscopic cholecystectomy.
{"title":"Influence of intercostal nerve block preemptive analgesia and incisional infiltration anesthesia on postoperative pain in patients undergoing laparoscopic cholecystectomy.","authors":"Ling Zhao, Yuxin Zhang, Xinde Chen, Chunyuan Zhang","doi":"10.1007/s00423-025-03816-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study is aiming at analyzing the effects of intercostal nerve block preemptive analgesia and incisional infiltration anesthesia on postoperative pain in patients undergoing laparoscopic cholecystectomy.</p><p><strong>Methods: </strong>Ninety patients who underwent laparoscopic cholecystectomy were retrospectively selected. According to different anesthesia methods, they were allocated into an intervention group and a control group, with 45 patients in each. The control group received incisional infiltration anesthesia alone, while the intervention group received intercostal nerve block with preemptive anesthesia combined with incisional infiltration. Pain intensity was assessed using the Visual Analogue Scale (VAS) at 4, 8, 12, and 24 h postoperatively at rest, and during mobilization at 8, 12, and 24 h. Postoperative analgesia conditions, as well as the operative time, length of hospital stay, time to first ambulation, and awakening time of the two groups, were compared. The incidence of adverse events was also compared.</p><p><strong>Results: </strong>The intervention group reported lower resting VAS scores at 4, 8, 12, and 24 h and lower movement-related VAS scores at 8, 12, and 24 h (all P < 0.05). The number of cases with VAS ≥ 4 at 4 h, 8 h, 12 h, and 24 h postoperatively in the control group was higher than that in the intervention group (P = 0.020, 0.033, 0.034, 0.019). Moreover, the proportion of patients who did not receive additional tramadol in the intervention group was higher at 4 h, 8 h, 12 h, and 24 h postoperatively [2/13 (15.38%) vs. 2/24 (8.33%); 5/16 (31.25%) vs. 3/28 (10.71%); 7/13 (53.85%) vs. 4/26 (15.38%); 4/10 (40.00%) vs. 3/22 (13.64%)]. There was no significant difference in the operative time between the two groups (P = 0.065). The length of hospital stay, time to first ambulation, and awakening time in the intervention group were all shorter than those in the control group (P < 0.05). The incidence of adverse events did not differ significantly between groups (8.89% vs. 13.33%, P = 0.739).</p><p><strong>Conclusion: </strong>Preemptive analgesia with intercostal nerve block & incisional infiltration anesthesia offers effective pain control in laparoscopic cholecystectomy, reducing the use of postoperative drugs, with a favorable safety profile.</p>","PeriodicalId":17983,"journal":{"name":"Langenbeck's Archives of Surgery","volume":"410 1","pages":"233"},"PeriodicalIF":1.8000,"publicationDate":"2025-07-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12310807/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Langenbeck's Archives of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00423-025-03816-3","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: This study is aiming at analyzing the effects of intercostal nerve block preemptive analgesia and incisional infiltration anesthesia on postoperative pain in patients undergoing laparoscopic cholecystectomy.
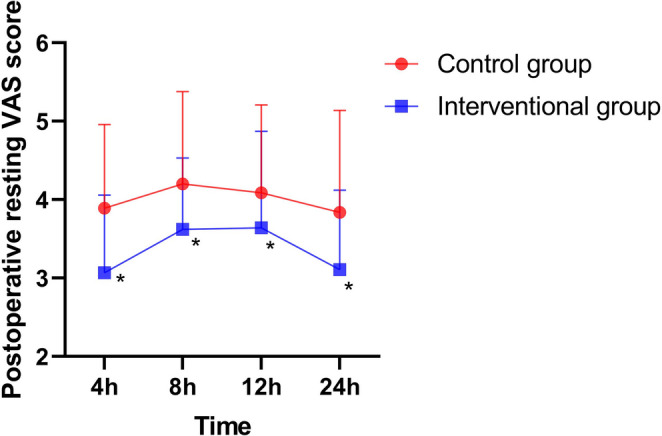
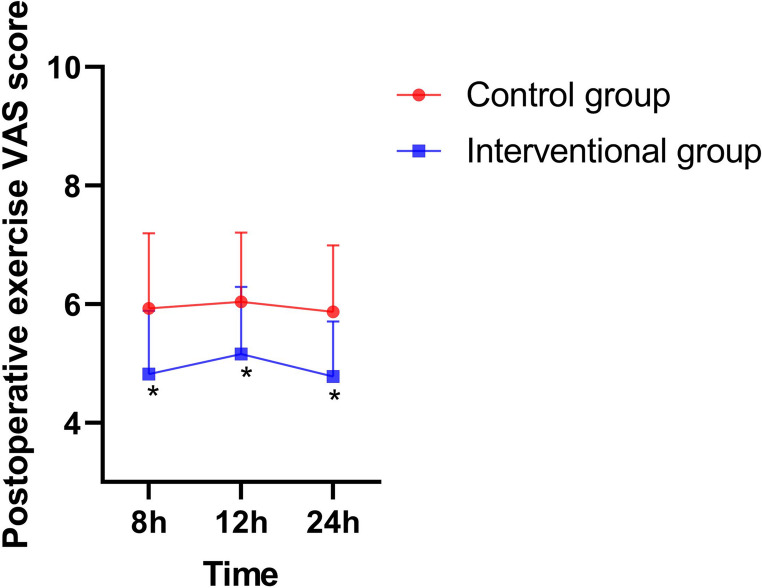
Methods: Ninety patients who underwent laparoscopic cholecystectomy were retrospectively selected. According to different anesthesia methods, they were allocated into an intervention group and a control group, with 45 patients in each. The control group received incisional infiltration anesthesia alone, while the intervention group received intercostal nerve block with preemptive anesthesia combined with incisional infiltration. Pain intensity was assessed using the Visual Analogue Scale (VAS) at 4, 8, 12, and 24 h postoperatively at rest, and during mobilization at 8, 12, and 24 h. Postoperative analgesia conditions, as well as the operative time, length of hospital stay, time to first ambulation, and awakening time of the two groups, were compared. The incidence of adverse events was also compared.
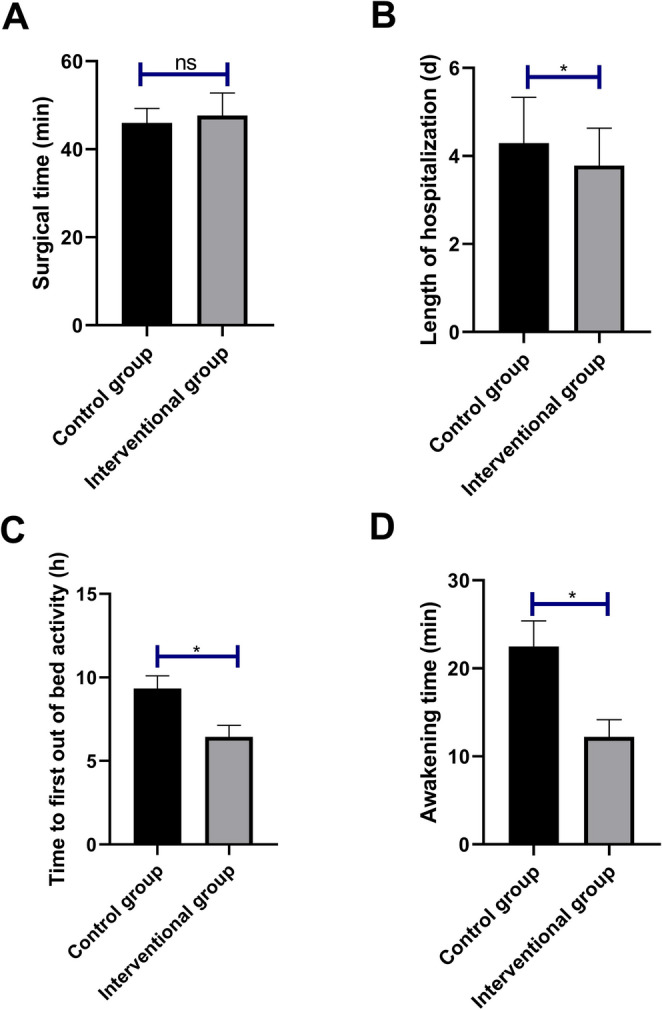
Results: The intervention group reported lower resting VAS scores at 4, 8, 12, and 24 h and lower movement-related VAS scores at 8, 12, and 24 h (all P < 0.05). The number of cases with VAS ≥ 4 at 4 h, 8 h, 12 h, and 24 h postoperatively in the control group was higher than that in the intervention group (P = 0.020, 0.033, 0.034, 0.019). Moreover, the proportion of patients who did not receive additional tramadol in the intervention group was higher at 4 h, 8 h, 12 h, and 24 h postoperatively [2/13 (15.38%) vs. 2/24 (8.33%); 5/16 (31.25%) vs. 3/28 (10.71%); 7/13 (53.85%) vs. 4/26 (15.38%); 4/10 (40.00%) vs. 3/22 (13.64%)]. There was no significant difference in the operative time between the two groups (P = 0.065). The length of hospital stay, time to first ambulation, and awakening time in the intervention group were all shorter than those in the control group (P < 0.05). The incidence of adverse events did not differ significantly between groups (8.89% vs. 13.33%, P = 0.739).
Conclusion: Preemptive analgesia with intercostal nerve block & incisional infiltration anesthesia offers effective pain control in laparoscopic cholecystectomy, reducing the use of postoperative drugs, with a favorable safety profile.
期刊介绍:
Langenbeck''s Archives of Surgery aims to publish the best results in the field of clinical surgery and basic surgical research. The main focus is on providing the highest level of clinical research and clinically relevant basic research. The journal, published exclusively in English, will provide an international discussion forum for the controlled results of clinical surgery. The majority of published contributions will be original articles reporting on clinical data from general and visceral surgery, while endocrine surgery will also be covered. Papers on basic surgical principles from the fields of traumatology, vascular and thoracic surgery are also welcome. Evidence-based medicine is an important criterion for the acceptance of papers.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


