Soraya Benamar, Cédric Lukas, Claire Daien, Cécile Gaujoux-Viala, Laure Gossec, Anne-Christine Rat, Bernard Combe, Jacques Morel
{"title":"Polypharmacy in Early Rheumatoid Arthritis: Impact on Treatment Response and Adverse Event Risk in a multicenter French prospective cohort study.","authors":"Soraya Benamar, Cédric Lukas, Claire Daien, Cécile Gaujoux-Viala, Laure Gossec, Anne-Christine Rat, Bernard Combe, Jacques Morel","doi":"10.1002/acr2.70066","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The objective of this study was to assess whether polypharmacy (PP) was associated with treatment response and serious adverse events (SAEs) in early rheumatoid arthritis (RA). Additionally, we aimed to investigate whether PP could serve as a surrogate marker for comorbidities.</p><p><strong>Methods: </strong>We used data from the French cohort ESPOIR, a prospective study of early RA. PP was defined as a categorical variable stratified into two or three categories according to median of distribution in the cohort. A logistic regression model was used. We assessed the occurrence of SAEs (severe infections, hospitalizations, deaths) throughout a 10-year follow-up period.</p><p><strong>Results: </strong>The proportion of patients who achieved DAS 28 remission (REM) one year after the initiation of the first disease-modifying antirheumatic drug (DMARD) was 32.1% in the PP group versus 67.9% in the non-PP group (P = 0.07) from 497 patients included. At five years, the proportion with REM was 45.0% in the PP group versus 56.3% in the non-PP group (P = 0.03). Patients taking two or more medications (excluding RA therapy) had a 40% lower likelihood of achieving REM at five years (adjusted odds ratio [OR] 0.60 [95% confidence interval (CI) 0.38-0.94], P = 0.03). At 10 years, patients receiving multiple medications had a 43% lower probability of achieving REM (adjusted OR 0.57 [95% CI 0.34-0.94], P = 0.02). The incidence of SAEs was 61 per 1,000 person-years. Among patients who developed SAEs, 86.4% were in the PP group and 49.8% were in the non-PP group (P = 0.03).</p><p><strong>Conclusion: </strong>PP is associated with a poorer treatment response and increased risk of SAEs. PP may serve as a good surrogate marker of comorbidities in epidemiologic studies.</p>","PeriodicalId":93845,"journal":{"name":"ACR open rheumatology","volume":"7 8","pages":"e70066"},"PeriodicalIF":2.8000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12305454/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACR open rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/acr2.70066","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The objective of this study was to assess whether polypharmacy (PP) was associated with treatment response and serious adverse events (SAEs) in early rheumatoid arthritis (RA). Additionally, we aimed to investigate whether PP could serve as a surrogate marker for comorbidities.
Methods: We used data from the French cohort ESPOIR, a prospective study of early RA. PP was defined as a categorical variable stratified into two or three categories according to median of distribution in the cohort. A logistic regression model was used. We assessed the occurrence of SAEs (severe infections, hospitalizations, deaths) throughout a 10-year follow-up period.
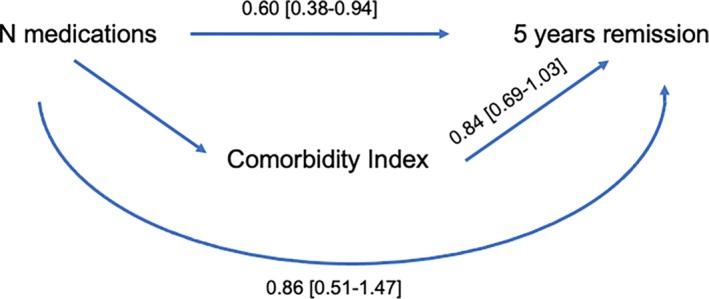
Results: The proportion of patients who achieved DAS 28 remission (REM) one year after the initiation of the first disease-modifying antirheumatic drug (DMARD) was 32.1% in the PP group versus 67.9% in the non-PP group (P = 0.07) from 497 patients included. At five years, the proportion with REM was 45.0% in the PP group versus 56.3% in the non-PP group (P = 0.03). Patients taking two or more medications (excluding RA therapy) had a 40% lower likelihood of achieving REM at five years (adjusted odds ratio [OR] 0.60 [95% confidence interval (CI) 0.38-0.94], P = 0.03). At 10 years, patients receiving multiple medications had a 43% lower probability of achieving REM (adjusted OR 0.57 [95% CI 0.34-0.94], P = 0.02). The incidence of SAEs was 61 per 1,000 person-years. Among patients who developed SAEs, 86.4% were in the PP group and 49.8% were in the non-PP group (P = 0.03).
Conclusion: PP is associated with a poorer treatment response and increased risk of SAEs. PP may serve as a good surrogate marker of comorbidities in epidemiologic studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


