Right ventricular uncoupling in acute heart failure with preserved or mildly reduced ejection fraction: a simple parameter to predict long-term mortality.
Lucrecia M Burgos, Lucía Campos Cervera, María A De Bortoli, Rocío C Baro Vila, Franco N Ballari, Mirta Diez
{"title":"Right ventricular uncoupling in acute heart failure with preserved or mildly reduced ejection fraction: a simple parameter to predict long-term mortality.","authors":"Lucrecia M Burgos, Lucía Campos Cervera, María A De Bortoli, Rocío C Baro Vila, Franco N Ballari, Mirta Diez","doi":"10.47487/apcyccv.v6i2.466","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Risk prediction in acute heart failure (AHF) has led to the development of multiple prognostic models. Emerging data highlight the prognostic significance of right ventricular (RV) to pulmonary artery (PA) uncoupling, which has been linked to adverse outcomes. Among patients with heart failure with preserved ejection fraction (HFpEF) and mildly reduced ejection fraction (HFmrEF), a highly heterogeneous group, the prognostic relevance of RV-PA uncoupling in forecasting long-term mortality is still not well defined. This study aimed to evaluate the association between RV-PA uncoupling and long-term mortality in a cohort of hospitalized HFpEF and HFmrEF patients.</p><p><strong>Materials and methods: </strong>We performed a retrospective analysis based on a prospective registry of adult patients admitted with a primary diagnosis of AHF between 2015 and 2020. Eligible patients had a left ventricular ejection fraction (LVEF) > 40%. The main outcome was all-cause mortality over long-term follow-up. RV-PA coupling was quantified using the ratio between tricuspid annular plane systolic excursion (TAPSE) and systolic pulmonary artery pressure (sPAP).</p><p><strong>Results: </strong>Out of 465 patients, simultaneous estimation of TAPSE and sPAP was feasible in 361 cases (77%). During a median follow-up of 20.9 months, 100 patients (27.7%) died. A TAPSE/sPAP ratio of 0.38 was identified as the optimal cut-off for risk discrimination. Notably, 41.8% of patients had values below this threshold. Multivariable analysis confirmed that RV-PA uncoupling (TAPSE/sPAP < 0.38) was independently associated with increased long-term mortality (HR: 2.21; 95% CI 1.26-3.81; P = 0.005).</p><p><strong>Conclusion: </strong>In patients hospitalized for AHF with preserved and mildly reduced ejection fraction, RV-PA uncoupling, as determined by the TAPSE/sPAP ratio, was independently associated with long-term all-cause mortality. This echocardiographic parameter may help identify a subgroup of patients at higher risk during follow-up.</p>","PeriodicalId":72295,"journal":{"name":"Archivos Peruanos de cardiologia y cirugia cardiovascular","volume":"6 2","pages":"83-89"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12288735/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archivos Peruanos de cardiologia y cirugia cardiovascular","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.47487/apcyccv.v6i2.466","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Risk prediction in acute heart failure (AHF) has led to the development of multiple prognostic models. Emerging data highlight the prognostic significance of right ventricular (RV) to pulmonary artery (PA) uncoupling, which has been linked to adverse outcomes. Among patients with heart failure with preserved ejection fraction (HFpEF) and mildly reduced ejection fraction (HFmrEF), a highly heterogeneous group, the prognostic relevance of RV-PA uncoupling in forecasting long-term mortality is still not well defined. This study aimed to evaluate the association between RV-PA uncoupling and long-term mortality in a cohort of hospitalized HFpEF and HFmrEF patients.
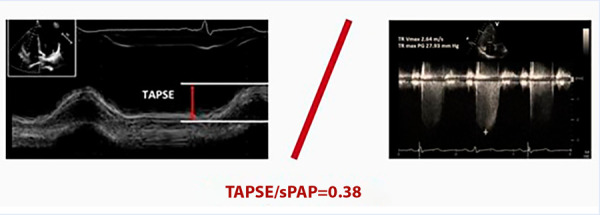
Materials and methods: We performed a retrospective analysis based on a prospective registry of adult patients admitted with a primary diagnosis of AHF between 2015 and 2020. Eligible patients had a left ventricular ejection fraction (LVEF) > 40%. The main outcome was all-cause mortality over long-term follow-up. RV-PA coupling was quantified using the ratio between tricuspid annular plane systolic excursion (TAPSE) and systolic pulmonary artery pressure (sPAP).
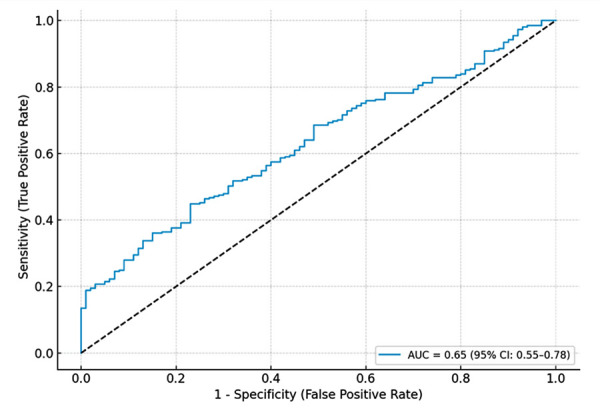
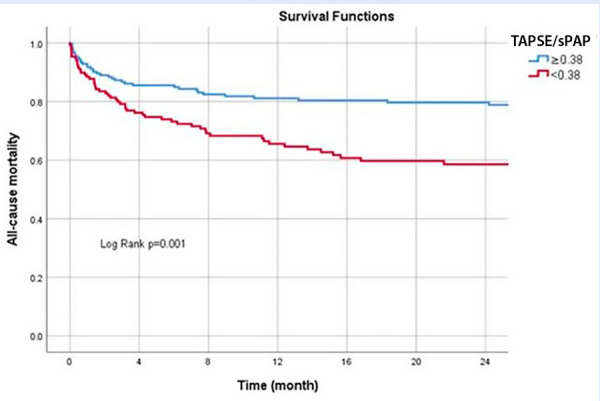
Results: Out of 465 patients, simultaneous estimation of TAPSE and sPAP was feasible in 361 cases (77%). During a median follow-up of 20.9 months, 100 patients (27.7%) died. A TAPSE/sPAP ratio of 0.38 was identified as the optimal cut-off for risk discrimination. Notably, 41.8% of patients had values below this threshold. Multivariable analysis confirmed that RV-PA uncoupling (TAPSE/sPAP < 0.38) was independently associated with increased long-term mortality (HR: 2.21; 95% CI 1.26-3.81; P = 0.005).
Conclusion: In patients hospitalized for AHF with preserved and mildly reduced ejection fraction, RV-PA uncoupling, as determined by the TAPSE/sPAP ratio, was independently associated with long-term all-cause mortality. This echocardiographic parameter may help identify a subgroup of patients at higher risk during follow-up.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


