Mollie R Cummins, Bob Wong, Neng Wan, Jiuying Han, Sukrut D Shishupal, Ramkiran Gouripeddi, Julia Ivanova, Asiyah Franklin, Jace Johnny, Triton Ong, Brandon M Welch, Brian E Bunnell
{"title":"Social vulnerability, lower broadband internet access, and rurality associated with lower telemedicine use in U.S. Counties.","authors":"Mollie R Cummins, Bob Wong, Neng Wan, Jiuying Han, Sukrut D Shishupal, Ramkiran Gouripeddi, Julia Ivanova, Asiyah Franklin, Jace Johnny, Triton Ong, Brandon M Welch, Brian E Bunnell","doi":"10.1093/jamiaopen/ooaf056","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Our objective was to determine how social vulnerabilities, broadband access, and rurality relate to telemedicine use across the United States through large-scale analysis of real-world telemedicine data.</p><p><strong>Materials and methods: </strong>We conducted a retrospective, observational study of dyadic U.S. telemedicine sessions that occurred January 1, 2022 to December 31, 2022, linked to the 2020 Centers for Disease Control and Prevention Social Vulnerability Index (SVI) and the National Center for Health Statistics Urban-Rural Classification Scheme for Counties. We examined county-level telemedicine use rates (sessions per 1000 population) in relation to SVI indexes, broadband internet access, and rurality classifications using polynomial regression and data visualization.</p><p><strong>Results: </strong>We found a negative, nonlinear association between overall social and socioeconomic status vulnerabilities and telemedicine use. Telemedicine rates in urban counties exceeded that of rural counties. There was more variability in telemedicine use for the urban counties according to social vulnerability and broadband access.</p><p><strong>Discussion: </strong>Rurality and broadband access demonstrated a greater effect on telemedicine use than social vulnerability, and the relationship between social vulnerability, broadband access, and telemedicine use differed for rural versus urban areas.</p><p><strong>Conclusion: </strong>This observational study of nearly 8 million U.S. telemedicine sessions showed that rurality and broadband access are key drivers of telemedicine use and may be more important than many social vulnerabilities in determining community-level telemedicine use. We also found nuanced differences in the relationship between social vulnerability and telemedicine use between rural and urban counties, and at different levels of broadband access.</p>","PeriodicalId":36278,"journal":{"name":"JAMIA Open","volume":"8 4","pages":"ooaf056"},"PeriodicalIF":3.4000,"publicationDate":"2025-07-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12296349/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMIA Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jamiaopen/ooaf056","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Our objective was to determine how social vulnerabilities, broadband access, and rurality relate to telemedicine use across the United States through large-scale analysis of real-world telemedicine data.
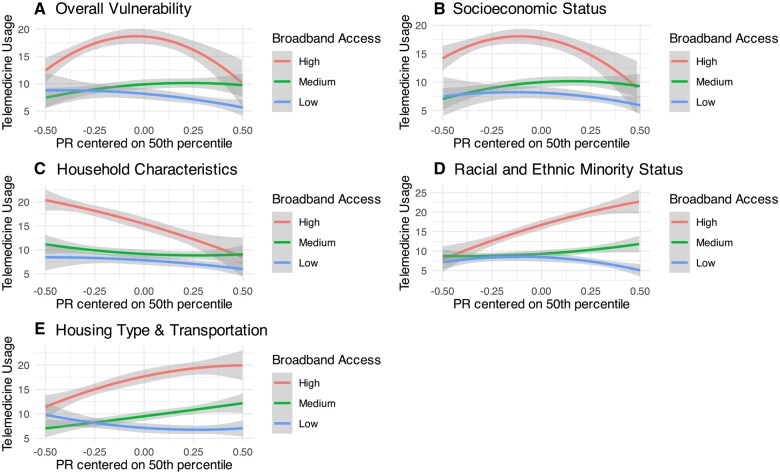
Materials and methods: We conducted a retrospective, observational study of dyadic U.S. telemedicine sessions that occurred January 1, 2022 to December 31, 2022, linked to the 2020 Centers for Disease Control and Prevention Social Vulnerability Index (SVI) and the National Center for Health Statistics Urban-Rural Classification Scheme for Counties. We examined county-level telemedicine use rates (sessions per 1000 population) in relation to SVI indexes, broadband internet access, and rurality classifications using polynomial regression and data visualization.
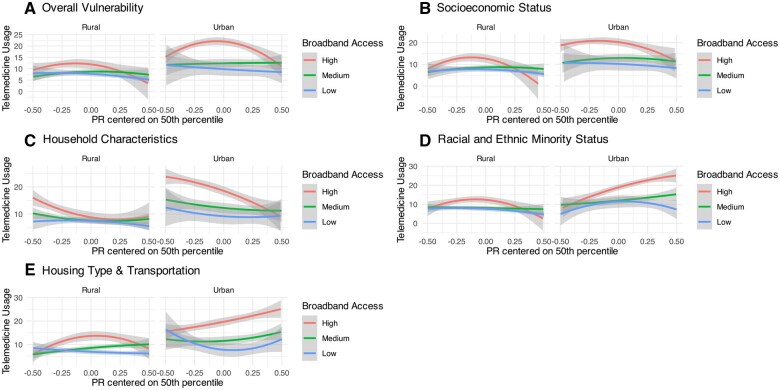
Results: We found a negative, nonlinear association between overall social and socioeconomic status vulnerabilities and telemedicine use. Telemedicine rates in urban counties exceeded that of rural counties. There was more variability in telemedicine use for the urban counties according to social vulnerability and broadband access.
Discussion: Rurality and broadband access demonstrated a greater effect on telemedicine use than social vulnerability, and the relationship between social vulnerability, broadband access, and telemedicine use differed for rural versus urban areas.
Conclusion: This observational study of nearly 8 million U.S. telemedicine sessions showed that rurality and broadband access are key drivers of telemedicine use and may be more important than many social vulnerabilities in determining community-level telemedicine use. We also found nuanced differences in the relationship between social vulnerability and telemedicine use between rural and urban counties, and at different levels of broadband access.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


