Caroline McCarthy, Barbara Clyne, Susan M Smith, Fiona Boland, Emma Wallace, Michelle Flood, Frank Moriarty
{"title":"Impact of eliciting treatment priorities on analgesic prescribing in older patients with high levels of polypharmacy.","authors":"Caroline McCarthy, Barbara Clyne, Susan M Smith, Fiona Boland, Emma Wallace, Michelle Flood, Frank Moriarty","doi":"10.1093/fampra/cmaf056","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Multimorbidity guidelines recommend tailoring care to patients' priorities. The Supporting Prescribing in Multimorbidity in Primary Care (SPPiRE) trial focused on optimizing medicines use in older adults with significant polypharmacy and tailoring prescribing and deprescribing to individual priorities. This study aimed to compare self-reported and general practitioner (GP)-recorded patient priorities and examine the impact of prioritizing pain on analgesic prescribing.</p><p><strong>Methods: </strong>This secondary cohort analysis of the SPPIRE trial and process evaluation assessed baseline participant-identified priorities and intervention group GP-recorded priorities during medication reviews with agreement assessed using Cohen's kappa. Analgesic prescribing patterns and daily morphine milligram equivalents changes during the study period were summarized. The impact of pain (self-reported, GP-recorded, and severe or extreme pain on the baseline EQ5D) on opioid intensification was analysed using multi-level models accounting for GP practice clustering and intervention effects.</p><p><strong>Results: </strong>A total of 403 patients (mean age 76.5 years) were included; 178 (44.2%) reported pain as a priority at baseline. Agreement between self-reported and GP-recorded pain was poor (kappa 0.118, P = 0.05). Most analgesic prescriptions decreased during the study, except for potent opioids, which increased in both trial arms. All three pain variables were associated with increased odds of opioid intensification at follow-up.</p><p><strong>Conclusion: </strong>In this older population of patients with significant polypharmacy, identifying pain as a priority was associated with an increased likelihood of opioid intensification, despite guidelines advising against their use for chronic pain. This study highlights the challenges faced by GPs treating pain in older adults with multimorbidity.</p>","PeriodicalId":12209,"journal":{"name":"Family practice","volume":"42 4","pages":""},"PeriodicalIF":2.2000,"publicationDate":"2025-06-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12302712/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Family practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/fampra/cmaf056","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Multimorbidity guidelines recommend tailoring care to patients' priorities. The Supporting Prescribing in Multimorbidity in Primary Care (SPPiRE) trial focused on optimizing medicines use in older adults with significant polypharmacy and tailoring prescribing and deprescribing to individual priorities. This study aimed to compare self-reported and general practitioner (GP)-recorded patient priorities and examine the impact of prioritizing pain on analgesic prescribing.
Methods: This secondary cohort analysis of the SPPIRE trial and process evaluation assessed baseline participant-identified priorities and intervention group GP-recorded priorities during medication reviews with agreement assessed using Cohen's kappa. Analgesic prescribing patterns and daily morphine milligram equivalents changes during the study period were summarized. The impact of pain (self-reported, GP-recorded, and severe or extreme pain on the baseline EQ5D) on opioid intensification was analysed using multi-level models accounting for GP practice clustering and intervention effects.
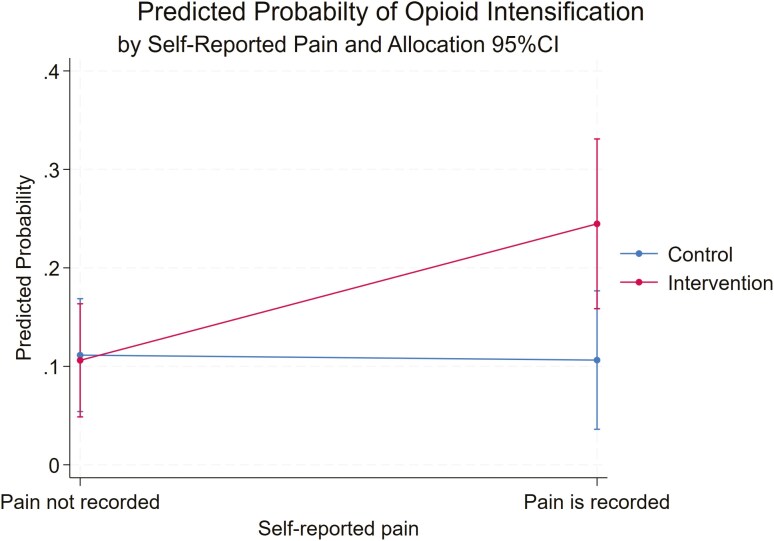
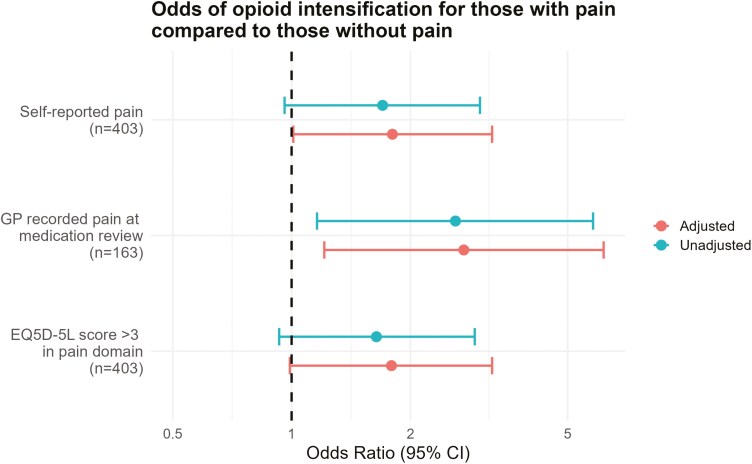
Results: A total of 403 patients (mean age 76.5 years) were included; 178 (44.2%) reported pain as a priority at baseline. Agreement between self-reported and GP-recorded pain was poor (kappa 0.118, P = 0.05). Most analgesic prescriptions decreased during the study, except for potent opioids, which increased in both trial arms. All three pain variables were associated with increased odds of opioid intensification at follow-up.
Conclusion: In this older population of patients with significant polypharmacy, identifying pain as a priority was associated with an increased likelihood of opioid intensification, despite guidelines advising against their use for chronic pain. This study highlights the challenges faced by GPs treating pain in older adults with multimorbidity.
期刊介绍:
Family Practice is an international journal aimed at practitioners, teachers, and researchers in the fields of family medicine, general practice, and primary care in both developed and developing countries.
Family Practice offers its readership an international view of the problems and preoccupations in the field, while providing a medium of instruction and exploration.
The journal''s range and content covers such areas as health care delivery, epidemiology, public health, and clinical case studies. The journal aims to be interdisciplinary and contributions from other disciplines of medicine and social science are always welcomed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


