Chang Liu, Jiashu Han, Renkui Fu, Tianyu Li, Georgios Antonios Margonis, Jaeyun Jane Wang, Kaiqi Ma, Weibin Wang, Chen Lin
{"title":"Timing of intravenous iron for treatment of anaemia in surgical patients: a systematic review and network meta-analysis.","authors":"Chang Liu, Jiashu Han, Renkui Fu, Tianyu Li, Georgios Antonios Margonis, Jaeyun Jane Wang, Kaiqi Ma, Weibin Wang, Chen Lin","doi":"10.1016/j.eclinm.2025.103361","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Anaemia complicates recovery in surgical patients. Intravenous (IV) iron supplementation shows promise in improving outcomes, but optimal timing remains uncertain. In this review, we compare the efficacy, safety, tolerability, and outcomes between preoperative and postoperative IV iron supplementation.</p><p><strong>Methods: </strong>In this systematic review and network meta-analysis, we searched PubMed, EMBASE, Cochrane Library, and Web of Science from inception to May 1, 2025, for randomised controlled trials (RCT) investigating IV iron supplementation in surgical patients either 7-30 days before surgery (preoperative) or 0-30 days after surgery (postoperative). Studies were excluded if they included patients with critical illness or prior transfusion or if iron was given outside the defined time frames or with other agents. Two reviewers independently appraised the data and extracted summary estimates from published reports. The primary outcomes were: (1) proportion of patients who received blood transfusion; (2) change between the baseline haemoglobin level and the haemoglobin level on postoperative day (POD) 7 and POD30. Data processing was conducted based on frequentist network meta-analysis. The risk of bias was assessed using the Cochrane Risk of Bias tool. The protocol is registered with PROSPERO, CRD42024533265.</p><p><strong>Findings: </strong>Among 129 identified studies, 22 RCTs with 3026 patients were included. All included studies had a low (n = 6) or moderate (n = 16) risk of bias. Compared to controls, postoperative IV iron supplementation reduced transfusion rates (RR 0.80, 95% CI 0.68-0.94; I<sup>2</sup> = 0.0%). Postoperative IV iron supplementation did not affect haemoglobin levels (MD -4.51, 95% CI -9.75 to 0.72; I<sup>2</sup> = 90.3%) at POD7 but increased haemoglobin levels (MD 5.45, 95% CI 2.70-8.20; I<sup>2</sup> = 45.5%) at POD30. In comparison, preoperative IV iron supplementation resulted in higher haemoglobin levels than postoperative supplementation at POD30 (MD 6.67, 95% CI 1.61-11.72) but did not influence transfusion rates (RR 0.91, 95% CI 0.72-1.15; I<sup>2</sup> = 0.0%).</p><p><strong>Interpretation: </strong>Our results suggest that postoperative IV iron supplementation reduces transfusion rates, while preoperative supplementation improves haemoglobin recovery. Clinicians may choose either strategy in an individualised, patient-centered manner. These conclusions should be interpreted with caution due to heterogeneity among included studies, limited data for subgroup analyses, and the absence of direct comparisons between preoperative and postoperative approaches.</p><p><strong>Funding: </strong>National Key Research and Development Program of China, National Natural Science Foundation of China, Beijing Natural Science Foundation, Capital's Funds for Health Improvement and Research, National High Level Hospital Clinical Research Funding, and Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences.</p>","PeriodicalId":11393,"journal":{"name":"EClinicalMedicine","volume":"86 ","pages":"103361"},"PeriodicalIF":10.0000,"publicationDate":"2025-07-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12303006/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"EClinicalMedicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.eclinm.2025.103361","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Anaemia complicates recovery in surgical patients. Intravenous (IV) iron supplementation shows promise in improving outcomes, but optimal timing remains uncertain. In this review, we compare the efficacy, safety, tolerability, and outcomes between preoperative and postoperative IV iron supplementation.
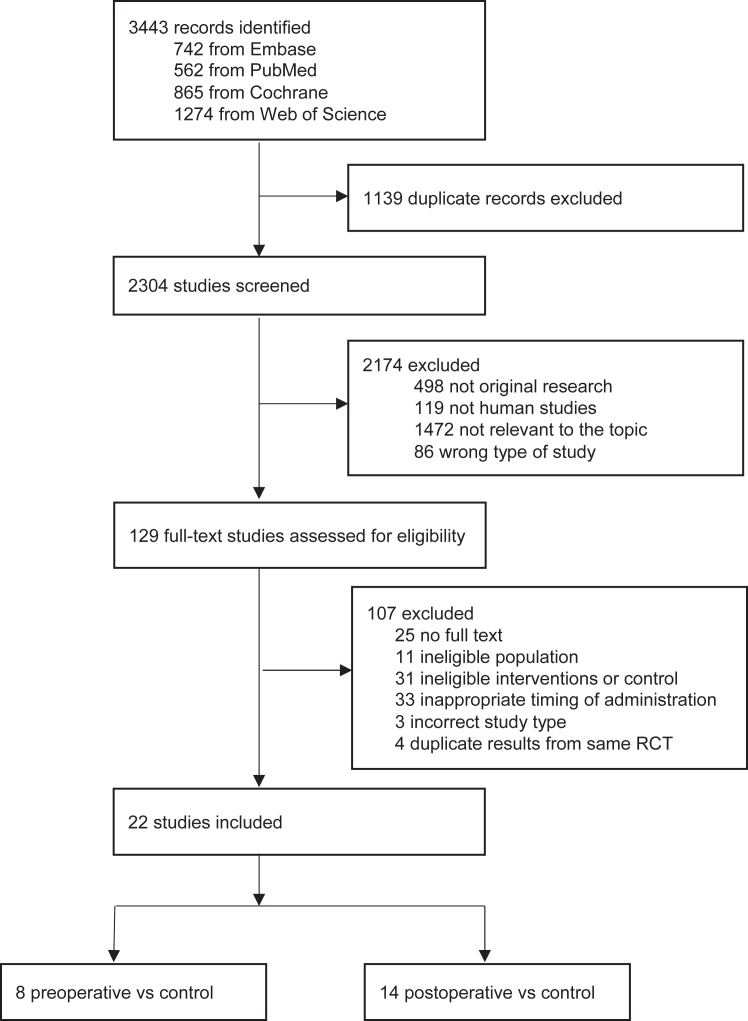
Methods: In this systematic review and network meta-analysis, we searched PubMed, EMBASE, Cochrane Library, and Web of Science from inception to May 1, 2025, for randomised controlled trials (RCT) investigating IV iron supplementation in surgical patients either 7-30 days before surgery (preoperative) or 0-30 days after surgery (postoperative). Studies were excluded if they included patients with critical illness or prior transfusion or if iron was given outside the defined time frames or with other agents. Two reviewers independently appraised the data and extracted summary estimates from published reports. The primary outcomes were: (1) proportion of patients who received blood transfusion; (2) change between the baseline haemoglobin level and the haemoglobin level on postoperative day (POD) 7 and POD30. Data processing was conducted based on frequentist network meta-analysis. The risk of bias was assessed using the Cochrane Risk of Bias tool. The protocol is registered with PROSPERO, CRD42024533265.
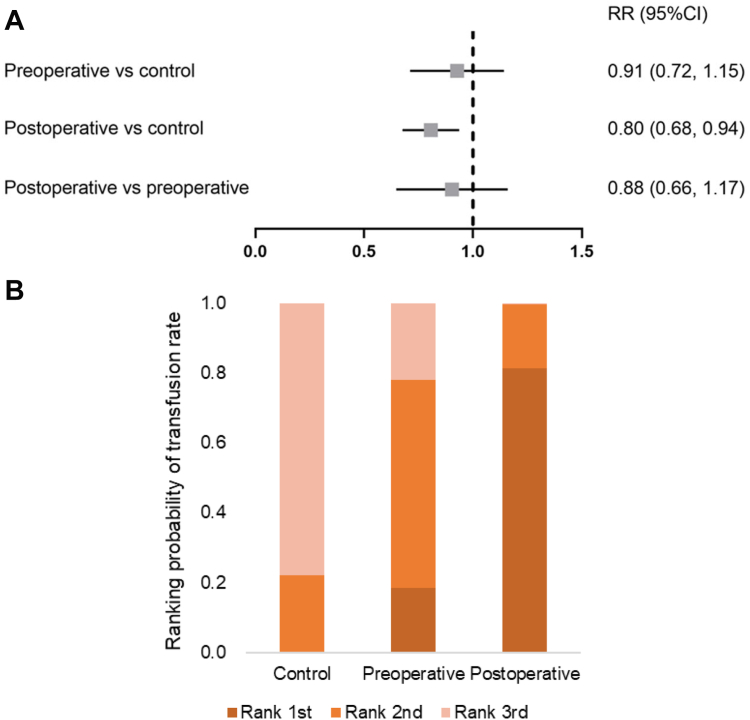
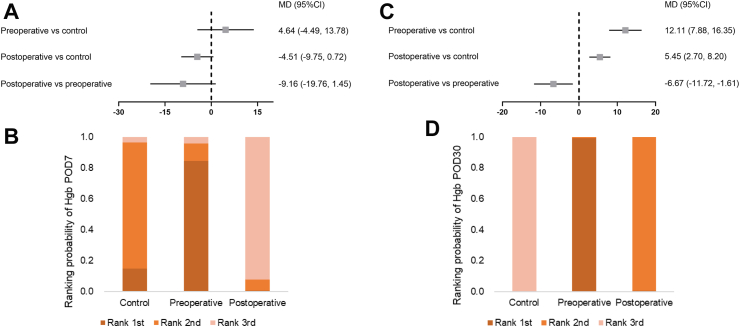
Findings: Among 129 identified studies, 22 RCTs with 3026 patients were included. All included studies had a low (n = 6) or moderate (n = 16) risk of bias. Compared to controls, postoperative IV iron supplementation reduced transfusion rates (RR 0.80, 95% CI 0.68-0.94; I2 = 0.0%). Postoperative IV iron supplementation did not affect haemoglobin levels (MD -4.51, 95% CI -9.75 to 0.72; I2 = 90.3%) at POD7 but increased haemoglobin levels (MD 5.45, 95% CI 2.70-8.20; I2 = 45.5%) at POD30. In comparison, preoperative IV iron supplementation resulted in higher haemoglobin levels than postoperative supplementation at POD30 (MD 6.67, 95% CI 1.61-11.72) but did not influence transfusion rates (RR 0.91, 95% CI 0.72-1.15; I2 = 0.0%).
Interpretation: Our results suggest that postoperative IV iron supplementation reduces transfusion rates, while preoperative supplementation improves haemoglobin recovery. Clinicians may choose either strategy in an individualised, patient-centered manner. These conclusions should be interpreted with caution due to heterogeneity among included studies, limited data for subgroup analyses, and the absence of direct comparisons between preoperative and postoperative approaches.
Funding: National Key Research and Development Program of China, National Natural Science Foundation of China, Beijing Natural Science Foundation, Capital's Funds for Health Improvement and Research, National High Level Hospital Clinical Research Funding, and Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences.
期刊介绍:
eClinicalMedicine is a gold open-access clinical journal designed to support frontline health professionals in addressing the complex and rapid health transitions affecting societies globally. The journal aims to assist practitioners in overcoming healthcare challenges across diverse communities, spanning diagnosis, treatment, prevention, and health promotion. Integrating disciplines from various specialties and life stages, it seeks to enhance health systems as fundamental institutions within societies. With a forward-thinking approach, eClinicalMedicine aims to redefine the future of healthcare.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


