Georgia Anne Santomartino, Kylie Crawford, Jesrine Hong, Sailesh Kumar
{"title":"Optimal timing and mode of planned birth for term, large infants: a retrospective, population-based cohort study.","authors":"Georgia Anne Santomartino, Kylie Crawford, Jesrine Hong, Sailesh Kumar","doi":"10.1016/j.eclinm.2025.103366","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Large infants (birthweight > 75th centile) are at increased risk of mortality, severe neonatal neurological and non-neurological morbidity. We aimed to ascertain the optimal method and gestation of planned birth (scheduled caesarean section or induction of labor) that were associated with lower odds of adverse outcomes.</p><p><strong>Methods: </strong>This was a retrospective cohort study of term singleton births with birthweight >75th centile between January 2000 and December 2021 in Queensland, Australia. Primary outcomes were severe adverse maternal outcome, perinatal mortality (intrapartum stillbirth or neonatal death), severe neonatal neurological morbidity, and other severe neonatal morbidity. Multivariable logistic regression models were built to determine odds ratios (OR) for the effect of timing of both methods of planned birth on adverse outcomes. Induction of labor at 38<sup>+0</sup>-38<sup>+6</sup> weeks was the referent category because many international guidelines recommend this as the optimum timing of birth.</p><p><strong>Findings: </strong>There were 151,464 planned births for large infants. 86,515 (57.1%) were induction of labor while 64,949 (42.9%) were scheduled caesarean section. Compared to induction of labor at 38<sup>+0</sup>-38<sup>+6</sup> weeks, induction at ≥41<sup>+0</sup> weeks (aOR 1.28, 95% CI 1.21, 1.35) and scheduled caesarean section at 37<sup>+0</sup>-37<sup>+6</sup> weeks (aOR 1.18, 95% CI 1.08, 1.28) were associated with greater odds of severe adverse maternal outcome, whilst scheduled caesarean section at 39<sup>+0</sup>-39<sup>+6</sup> weeks (aOR 0.75, 95% CI 0.70, 0.80) was associated with lower odds of this outcome. The odds of severe neonatal neurological morbidity were lower following induction at 40<sup>+0</sup>-40<sup>+6</sup> weeks (aOR 0.72, 95% CI 0.59, 0.89) or scheduled caesarean section at 37<sup>+0</sup>-37<sup>+6</sup> weeks (aOR 0.59, 95% CI 0.43, 0.81), 39<sup>+0</sup>-39<sup>+6</sup> weeks (aOR 0.26, 95% CI 0.2, 0.33), and ≥41<sup>+0</sup> weeks (aOR 0.31, 95% CI 0.13, 0.75) respectively. For other severe neonatal morbidity, the odds were highest after induction of labor at 37<sup>+0</sup>-37<sup>+6</sup> weeks (aOR 1.35, 95% CI 1.24, 1.46), and lowest following scheduled caesarean section at 40<sup>+0</sup>-40<sup>+6</sup> weeks (aOR 0.31, 95% CI 0.26, 0.36). There were no significant differences in perinatal mortality based on method of planned birth or gestational age.</p><p><strong>Interpretation: </strong>In our cohort, scheduled caesarean section between 39<sup>+0</sup>-39<sup>+6</sup> weeks for large infants at birth was associated with lower odds of severe adverse maternal outcomes, severe neonatal neurological morbidity, and other severe neonatal morbidity compared to induction of labor at 38<sup>+0</sup>-38<sup>+6</sup> weeks. For women that underwent induction of labor, the odds of emergency caesarean section were lowest at 39<sup>+0</sup>-39<sup>+6</sup> weeks. Infants with birthweight >97th centile for gestational age had the highest risk of adverse outcomes regardless of gestation or method of planned birth.</p><p><strong>Funding: </strong>National Health and Medical Research Council and Mater Foundation.</p>","PeriodicalId":11393,"journal":{"name":"EClinicalMedicine","volume":"86 ","pages":"103366"},"PeriodicalIF":10.0000,"publicationDate":"2025-07-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12302999/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"EClinicalMedicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.eclinm.2025.103366","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Large infants (birthweight > 75th centile) are at increased risk of mortality, severe neonatal neurological and non-neurological morbidity. We aimed to ascertain the optimal method and gestation of planned birth (scheduled caesarean section or induction of labor) that were associated with lower odds of adverse outcomes.
Methods: This was a retrospective cohort study of term singleton births with birthweight >75th centile between January 2000 and December 2021 in Queensland, Australia. Primary outcomes were severe adverse maternal outcome, perinatal mortality (intrapartum stillbirth or neonatal death), severe neonatal neurological morbidity, and other severe neonatal morbidity. Multivariable logistic regression models were built to determine odds ratios (OR) for the effect of timing of both methods of planned birth on adverse outcomes. Induction of labor at 38+0-38+6 weeks was the referent category because many international guidelines recommend this as the optimum timing of birth.
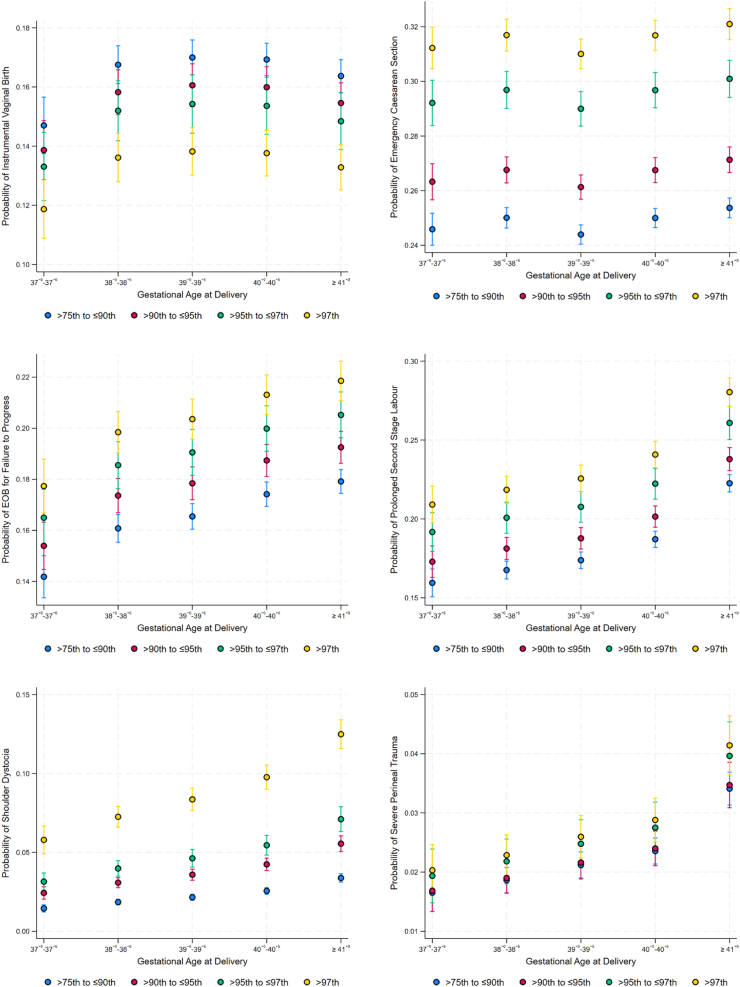
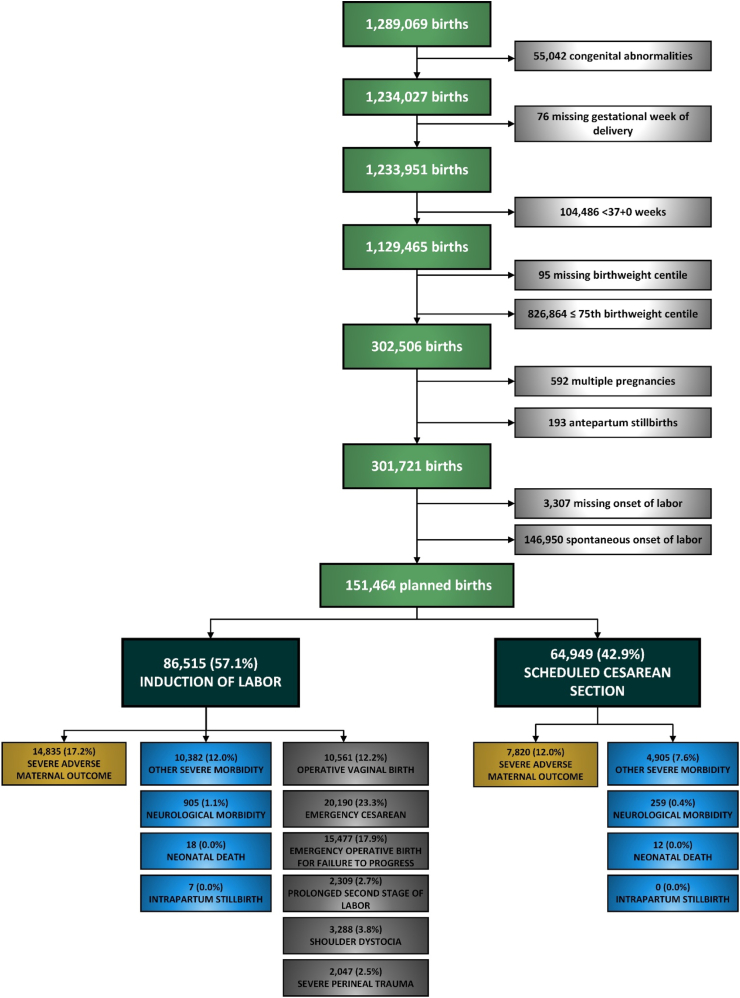
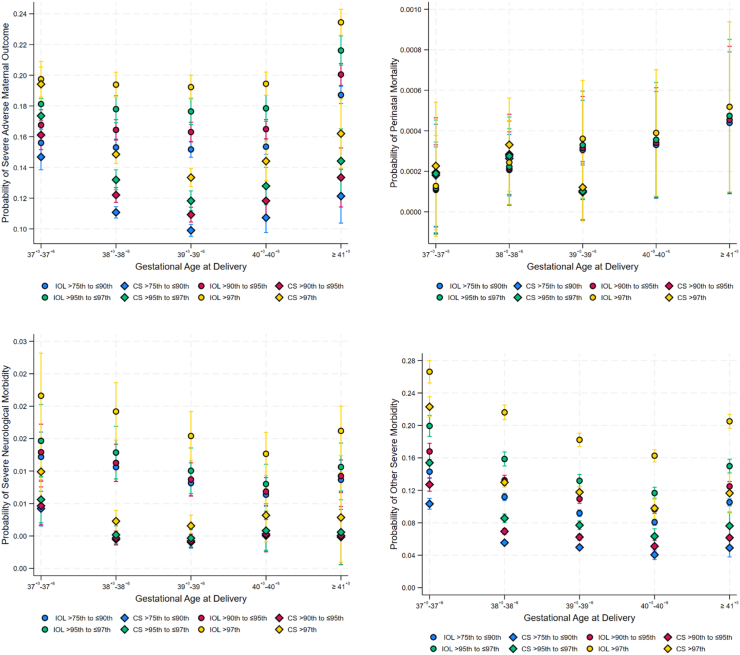
Findings: There were 151,464 planned births for large infants. 86,515 (57.1%) were induction of labor while 64,949 (42.9%) were scheduled caesarean section. Compared to induction of labor at 38+0-38+6 weeks, induction at ≥41+0 weeks (aOR 1.28, 95% CI 1.21, 1.35) and scheduled caesarean section at 37+0-37+6 weeks (aOR 1.18, 95% CI 1.08, 1.28) were associated with greater odds of severe adverse maternal outcome, whilst scheduled caesarean section at 39+0-39+6 weeks (aOR 0.75, 95% CI 0.70, 0.80) was associated with lower odds of this outcome. The odds of severe neonatal neurological morbidity were lower following induction at 40+0-40+6 weeks (aOR 0.72, 95% CI 0.59, 0.89) or scheduled caesarean section at 37+0-37+6 weeks (aOR 0.59, 95% CI 0.43, 0.81), 39+0-39+6 weeks (aOR 0.26, 95% CI 0.2, 0.33), and ≥41+0 weeks (aOR 0.31, 95% CI 0.13, 0.75) respectively. For other severe neonatal morbidity, the odds were highest after induction of labor at 37+0-37+6 weeks (aOR 1.35, 95% CI 1.24, 1.46), and lowest following scheduled caesarean section at 40+0-40+6 weeks (aOR 0.31, 95% CI 0.26, 0.36). There were no significant differences in perinatal mortality based on method of planned birth or gestational age.
Interpretation: In our cohort, scheduled caesarean section between 39+0-39+6 weeks for large infants at birth was associated with lower odds of severe adverse maternal outcomes, severe neonatal neurological morbidity, and other severe neonatal morbidity compared to induction of labor at 38+0-38+6 weeks. For women that underwent induction of labor, the odds of emergency caesarean section were lowest at 39+0-39+6 weeks. Infants with birthweight >97th centile for gestational age had the highest risk of adverse outcomes regardless of gestation or method of planned birth.
Funding: National Health and Medical Research Council and Mater Foundation.
期刊介绍:
eClinicalMedicine is a gold open-access clinical journal designed to support frontline health professionals in addressing the complex and rapid health transitions affecting societies globally. The journal aims to assist practitioners in overcoming healthcare challenges across diverse communities, spanning diagnosis, treatment, prevention, and health promotion. Integrating disciplines from various specialties and life stages, it seeks to enhance health systems as fundamental institutions within societies. With a forward-thinking approach, eClinicalMedicine aims to redefine the future of healthcare.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


