Emily P Hyle, Thulani Maphosa, Ajay Rangaraj, Mary Feser, Geoffrey C Singini, Prakriti Shrestha, Amir Shroufi, Krishna P Reddy, Eddie Matiya, Rosalia Dambe, Virginia R Talbot, Rachel Chamanga, C Robert Horsburgh, Milton C Weinstein, Rose K Nyirenda, Nathan Ford, Appolinaire Tiam, Andrew Phillips, Kenneth A Freedberg
{"title":"Clinical impact and cost-effectiveness of the WHO-recommended advanced HIV disease package of care.","authors":"Emily P Hyle, Thulani Maphosa, Ajay Rangaraj, Mary Feser, Geoffrey C Singini, Prakriti Shrestha, Amir Shroufi, Krishna P Reddy, Eddie Matiya, Rosalia Dambe, Virginia R Talbot, Rachel Chamanga, C Robert Horsburgh, Milton C Weinstein, Rose K Nyirenda, Nathan Ford, Appolinaire Tiam, Andrew Phillips, Kenneth A Freedberg","doi":"10.1016/S2214-109X(25)00190-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In sub-Saharan Africa, 20-40% of people living with HIV present with advanced HIV disease (AHD), which can be diagnosed, treated, and prevented using a package of care recommended by WHO. We aimed to project the cost-effectiveness and budget impact of the WHO-recommended AHD package in Malawi.</p><p><strong>Methods: </strong>Using the Cost-Effectiveness of Preventing AIDS Complications-International model, we simulated a cohort of non-hospitalised people living with HIV (aged >19 years) initiating antiretroviral therapy (ART), 25% of whom had AHD (CD4 count <200 cells per μL and/or WHO stage 3 or 4 disease). We assessed 13 increasingly comprehensive strategies, ranging from ART only to the WHO-recommended AHD package, including tuberculosis diagnostics (ie, sputum Xpert and urine lipoarabinomannan), tuberculosis preventive therapy, serum cryptococcal antigen (CrAg) screening with pre-emptive fluconazole treatment if CrAg-positive, and co-trimoxazole to prevent bacterial infections. Model outcomes included 1 year survival, life expectancy, costs, and incremental cost-effectiveness ratios (ICERs, US$ per quality-adjusted life-year [QALY]); we considered a strategy cost-effective if the ICER was less than $600 per QALY (based on 2023 Malawi per capita gross domestic product).</p><p><strong>Findings: </strong>ART only resulted in life expectancy of 17·45 undiscounted QALYs and discounted lifetime costs of $1450. All other strategies would increase both QALYs and costs. The WHO-recommended AHD package would result in the greatest life expectancy (19·30 undiscounted QALYs) and be cost-effective (ICER $580 per QALY). AHD prevalence and intervention efficacy had the greatest influence on ICERs; however, the WHO-recommended AHD package would remain cost-effective over a wide range of estimates.</p><p><strong>Interpretation: </strong>The WHO-recommended AHD package of care at ART initiation would provide substantial clinical benefits and be cost-effective in Malawi. This package for AHD should be made widely available in Malawi and similar settings.</p><p><strong>Funding: </strong>WHO, the HIV Modelling Consortium within the Institute for Global Health at University College London, the Bill & Melinda Gates Foundation, the National Institute of Allergy and Infectious Diseases, the Massachusetts General Hospital Jerome and Celia Reich Endowed Scholar in HIV/AIDS Research Award, and the Steve and Deborah Gorlin Massachusetts General Hospital Research Scholars Award.</p><p><strong>Translation: </strong>For the Chichewa translation of the abstract see Supplementary Materials section.</p>","PeriodicalId":48783,"journal":{"name":"Lancet Global Health","volume":"13 8","pages":"e1436-e1447"},"PeriodicalIF":19.9000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12286912/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Lancet Global Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/S2214-109X(25)00190-1","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In sub-Saharan Africa, 20-40% of people living with HIV present with advanced HIV disease (AHD), which can be diagnosed, treated, and prevented using a package of care recommended by WHO. We aimed to project the cost-effectiveness and budget impact of the WHO-recommended AHD package in Malawi.
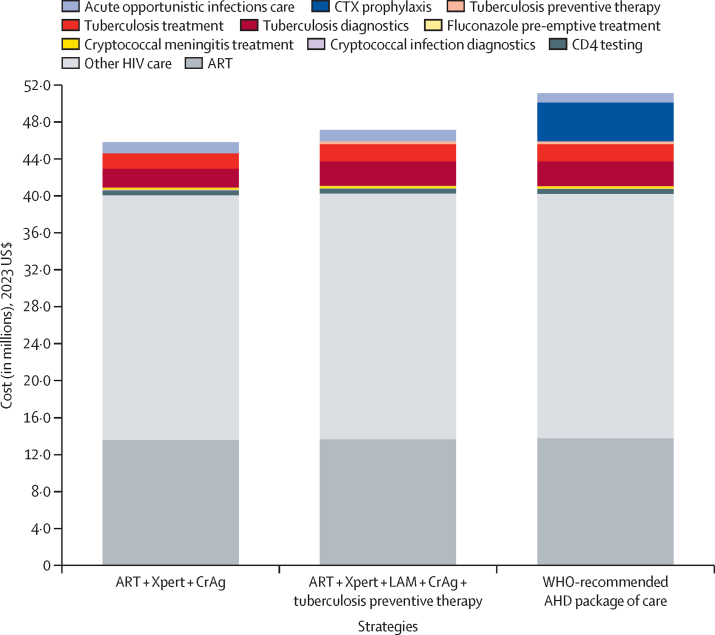
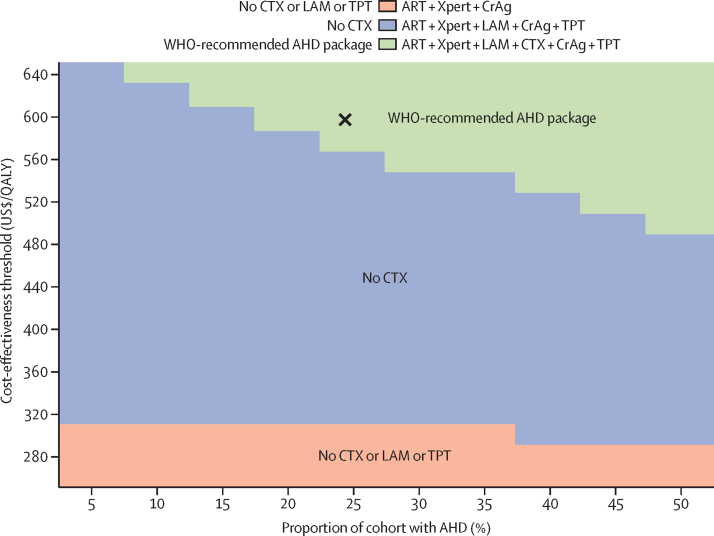
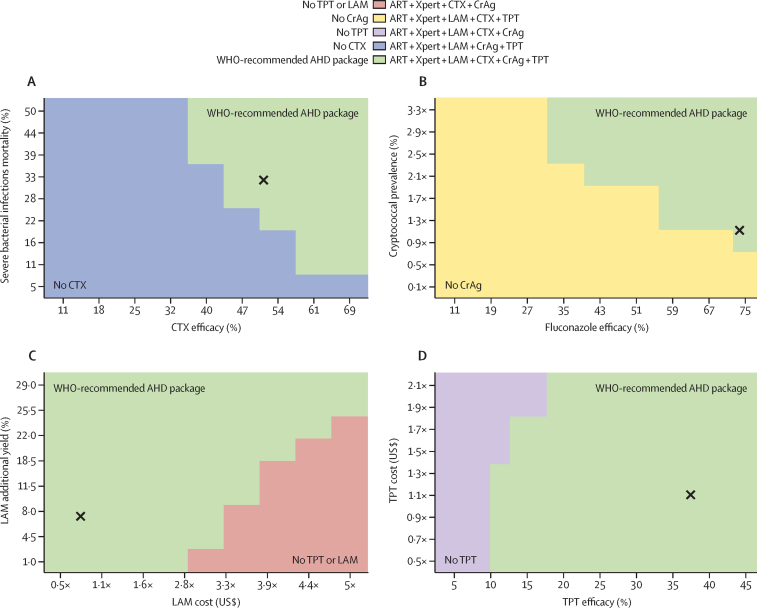
Methods: Using the Cost-Effectiveness of Preventing AIDS Complications-International model, we simulated a cohort of non-hospitalised people living with HIV (aged >19 years) initiating antiretroviral therapy (ART), 25% of whom had AHD (CD4 count <200 cells per μL and/or WHO stage 3 or 4 disease). We assessed 13 increasingly comprehensive strategies, ranging from ART only to the WHO-recommended AHD package, including tuberculosis diagnostics (ie, sputum Xpert and urine lipoarabinomannan), tuberculosis preventive therapy, serum cryptococcal antigen (CrAg) screening with pre-emptive fluconazole treatment if CrAg-positive, and co-trimoxazole to prevent bacterial infections. Model outcomes included 1 year survival, life expectancy, costs, and incremental cost-effectiveness ratios (ICERs, US$ per quality-adjusted life-year [QALY]); we considered a strategy cost-effective if the ICER was less than $600 per QALY (based on 2023 Malawi per capita gross domestic product).
Findings: ART only resulted in life expectancy of 17·45 undiscounted QALYs and discounted lifetime costs of $1450. All other strategies would increase both QALYs and costs. The WHO-recommended AHD package would result in the greatest life expectancy (19·30 undiscounted QALYs) and be cost-effective (ICER $580 per QALY). AHD prevalence and intervention efficacy had the greatest influence on ICERs; however, the WHO-recommended AHD package would remain cost-effective over a wide range of estimates.
Interpretation: The WHO-recommended AHD package of care at ART initiation would provide substantial clinical benefits and be cost-effective in Malawi. This package for AHD should be made widely available in Malawi and similar settings.
Funding: WHO, the HIV Modelling Consortium within the Institute for Global Health at University College London, the Bill & Melinda Gates Foundation, the National Institute of Allergy and Infectious Diseases, the Massachusetts General Hospital Jerome and Celia Reich Endowed Scholar in HIV/AIDS Research Award, and the Steve and Deborah Gorlin Massachusetts General Hospital Research Scholars Award.
Translation: For the Chichewa translation of the abstract see Supplementary Materials section.
期刊介绍:
The Lancet Global Health is an online publication that releases monthly open access (subscription-free) issues.Each issue includes original research, commentary, and correspondence.In addition to this, the publication also provides regular blog posts.
The main focus of The Lancet Global Health is on disadvantaged populations, which can include both entire economic regions and marginalized groups within prosperous nations.The publication prefers to cover topics related to reproductive, maternal, neonatal, child, and adolescent health; infectious diseases (including neglected tropical diseases); non-communicable diseases; mental health; the global health workforce; health systems; surgery; and health policy.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


