Performance of dispatcher-assisted cardiopulmonary resuscitation integrating with mouth-and-nose covering instructions during the COVID-19 pandemic: a population-based retrospective study.
{"title":"Performance of dispatcher-assisted cardiopulmonary resuscitation integrating with mouth-and-nose covering instructions during the COVID-19 pandemic: a population-based retrospective study.","authors":"Hideki Asai, Hidetada Fukushima, Yasuyuki Kawai, Keita Miyazaki, Kouji Yamamoto, Arisa Kinoshita, Hirozumi Okuda","doi":"10.1186/s12873-025-01296-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The coronavirus disease 2019 (COVID-19) pandemic, which emerged in late 2019, compelled people to change their behavior globally. Due to concerns about potential aerosol transmission during chest compressions, a modified dispatcher-assisted cardiopulmonary resuscitation (DACPR) protocol incorporating mouth-and-nose covering instructions was introduced in Nara, Japan. This study examined its impact on DACPR performance during the COVID-19 pandemic.</p><p><strong>Methods: </strong>This is a retrospective before-after study. DACPR performance data from the Nara Wide Area Fire Department were analyzed, comparing the non-pandemic period (March 2019 to February 2020) with the pandemic period (November 2020 to October 2021). The primary outcome was the time from emergency call acceptance to the first chest compression (T3). Secondary outcomes included the time to cardiac arrest recognition (T1), the time to start of DACPR instructions (T2), DACPR implementation rate, and adherence to infection prevention instructions.</p><p><strong>Results: </strong>The implementation of the modified protocol did not significantly alter the overall DACPR rate (406, 50.3% in the non-pandemic vs. 390, 47.2% in the pandemic; p =.214). Although the difference was relatively small, a statistically significant prolongation of T3 was observed during the pandemic period (246.0 s vs. 261.5 s, p <.05). Compliance with mouth-and-nose covering instructions among dispatchers was relatively low (43.1%). Among cases where such instructions were provided, only 21.4% of bystanders fully adhered to the protocol (both the bystander and the patient covering their mouth and nose). However, dispatcher-provided instructions significantly increased the likelihood of bystanders wearing masks and covering the patient's mouth and nose. Multivariable analysis did not identify the protocol implementation as a significant factor influencing T3.</p><p><strong>Conclusions: </strong>This study demonstrated that the modified DACPR protocol incorporating infection prevention measures was associated with a statistically significant delay of approximately 15.0 s in CPR initiation. However, given the low adherence rate, the overall impact of these measures on DACPR performance was limited. These findings highlight the need to increase adherence to infection prevention measures while minimizing delays in life-saving interventions, particularly during pandemics caused by airborne pathogens.</p>","PeriodicalId":9002,"journal":{"name":"BMC Emergency Medicine","volume":"25 1","pages":"134"},"PeriodicalIF":2.3000,"publicationDate":"2025-07-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12296633/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12873-025-01296-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The coronavirus disease 2019 (COVID-19) pandemic, which emerged in late 2019, compelled people to change their behavior globally. Due to concerns about potential aerosol transmission during chest compressions, a modified dispatcher-assisted cardiopulmonary resuscitation (DACPR) protocol incorporating mouth-and-nose covering instructions was introduced in Nara, Japan. This study examined its impact on DACPR performance during the COVID-19 pandemic.
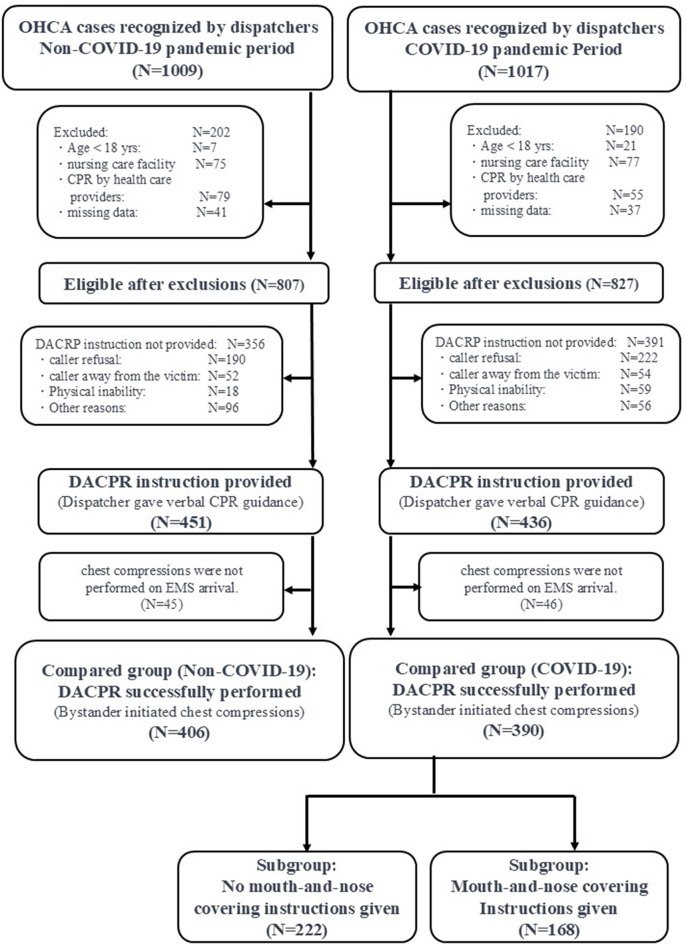
Methods: This is a retrospective before-after study. DACPR performance data from the Nara Wide Area Fire Department were analyzed, comparing the non-pandemic period (March 2019 to February 2020) with the pandemic period (November 2020 to October 2021). The primary outcome was the time from emergency call acceptance to the first chest compression (T3). Secondary outcomes included the time to cardiac arrest recognition (T1), the time to start of DACPR instructions (T2), DACPR implementation rate, and adherence to infection prevention instructions.
Results: The implementation of the modified protocol did not significantly alter the overall DACPR rate (406, 50.3% in the non-pandemic vs. 390, 47.2% in the pandemic; p =.214). Although the difference was relatively small, a statistically significant prolongation of T3 was observed during the pandemic period (246.0 s vs. 261.5 s, p <.05). Compliance with mouth-and-nose covering instructions among dispatchers was relatively low (43.1%). Among cases where such instructions were provided, only 21.4% of bystanders fully adhered to the protocol (both the bystander and the patient covering their mouth and nose). However, dispatcher-provided instructions significantly increased the likelihood of bystanders wearing masks and covering the patient's mouth and nose. Multivariable analysis did not identify the protocol implementation as a significant factor influencing T3.
Conclusions: This study demonstrated that the modified DACPR protocol incorporating infection prevention measures was associated with a statistically significant delay of approximately 15.0 s in CPR initiation. However, given the low adherence rate, the overall impact of these measures on DACPR performance was limited. These findings highlight the need to increase adherence to infection prevention measures while minimizing delays in life-saving interventions, particularly during pandemics caused by airborne pathogens.
背景:2019年底出现的2019冠状病毒病(COVID-19)大流行迫使全球人们改变自己的行为。由于对胸外按压过程中可能出现的气溶胶传播的担忧,日本奈良引入了一种经过修改的调度员辅助心肺复苏(DACPR)方案,其中包括捂住口鼻的说明。本研究考察了其在COVID-19大流行期间对DACPR性能的影响。方法:回顾性前后对照研究。分析了奈良广域消防局的DACPR绩效数据,将非大流行时期(2019年3月至2020年2月)与大流行时期(2020年11月至2021年10月)进行了比较。主要观察指标为从接受急诊呼叫到首次胸外按压(T3)的时间。次要结局包括心脏骤停识别时间(T1)、开始DACPR指令时间(T2)、DACPR执行率和对感染预防指令的依从性。结果:修改方案的实施并未显著改变总体DACPR率(非大流行组为406.50.3%,大流行组为39047.2%;p = .214)。虽然差异相对较小,但在大流行期间观察到T3的延长具有统计学意义(246.0 s vs 261.5 s, p)。结论:本研究表明,纳入感染预防措施的修改后的DACPR方案与CPR启动延迟约15.0 s具有统计学意义。然而,鉴于低依从率,这些措施对DACPR性能的总体影响是有限的。这些发现突出表明,需要加强对感染预防措施的遵守,同时尽量减少挽救生命的干预措施的延误,特别是在由空气传播病原体引起的大流行期间。
期刊介绍:
BMC Emergency Medicine is an open access, peer-reviewed journal that considers articles on all urgent and emergency aspects of medicine, in both practice and basic research. In addition, the journal covers aspects of disaster medicine and medicine in special locations, such as conflict areas and military medicine, together with articles concerning healthcare services in the emergency departments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


