{"title":"Assessment of SARC-F Sensitivity for Probable Sarcopenia Among Community-Dwelling Older Adults: Cross-Sectional Questionnaire Study.","authors":"David Propst, Lauren Biscardi, Tim Dornemann","doi":"10.2196/54475","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The European Working Group on Sarcopenia in Older People (EWGSOP2) recommends the use of the 5-item SARC-F (strength, assistance with walking, rising from a chair, climbing stairs, and falls) questionnaire by clinicians to screen for probable sarcopenia. The recommended threshold of ≥4 has low sensitivity and high specificity in identifying probable sarcopenia. While this high threshold is effective in excluding clients without probable sarcopenia, challenges exist in using this screening tool to identify clients with low muscle strength.</p><p><strong>Objective: </strong>This study aims to reassess the use of SARC-F in a primary care clinic for the determination of incidence of probable sarcopenia and to evaluate if a handgrip strength test is necessary for its diagnosis.</p><p><strong>Methods: </strong>We screened 204 patients aged ≥65 years (117 men and 87 women) during routine visits with the SARC-F questionnaire. Probable sarcopenia was defined by EWGSOP2 grip strength cut points (≤27 kg for men and ≤16 kg for women). Receiver operating characteristic analysis was performed to identify the SARC-F threshold that best balanced sensitivity and specificity.</p><p><strong>Results: </strong>Probable sarcopenia was present in 12% (n=24) of participants. The mean age (73.9, SD 6.2 years) and mean BMI (29.5, SD 5.8 kg/m²) did not differ significantly by sex; however, men showed a higher mean grip strength (36.3, SD 8.1 kg vs 22.4, SD 5.5 kg; P<.001) and lower mean SARC-F scores (0.9, SD 1.7 vs 1.9, SD 2.3; P<.001). A SARC-F cut point of ≥2 yielded an area under the curve of 0.77 (95% CI 0.67-0.88), with sensitivity of 0.78, specificity of 0.75, accuracy of 0.77, positive predictive value of 0.31, and negative predictive value of 0.96. The grip strength differed significantly between screen-positive and screen-negative groups at both the ≥2 and ≥4 thresholds (P<.001).</p><p><strong>Conclusions: </strong>A SARC- F threshold of ≥2 is recommended as an optimal trade-off between sensitivity and specificity for identifying community-dwelling older adults with probable sarcopenia. This threshold is lower than the currently accepted recommendation of ≥4. Our findings promote the recommendations for early detection and treatment by medical professionals following the EWGSOP2 by improving the ability of clinicians to identify individuals with low muscle strength using this screening procedure.</p>","PeriodicalId":73558,"journal":{"name":"JMIRx med","volume":"6 ","pages":"e54475"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12292031/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIRx med","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/54475","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The European Working Group on Sarcopenia in Older People (EWGSOP2) recommends the use of the 5-item SARC-F (strength, assistance with walking, rising from a chair, climbing stairs, and falls) questionnaire by clinicians to screen for probable sarcopenia. The recommended threshold of ≥4 has low sensitivity and high specificity in identifying probable sarcopenia. While this high threshold is effective in excluding clients without probable sarcopenia, challenges exist in using this screening tool to identify clients with low muscle strength.
Objective: This study aims to reassess the use of SARC-F in a primary care clinic for the determination of incidence of probable sarcopenia and to evaluate if a handgrip strength test is necessary for its diagnosis.
Methods: We screened 204 patients aged ≥65 years (117 men and 87 women) during routine visits with the SARC-F questionnaire. Probable sarcopenia was defined by EWGSOP2 grip strength cut points (≤27 kg for men and ≤16 kg for women). Receiver operating characteristic analysis was performed to identify the SARC-F threshold that best balanced sensitivity and specificity.
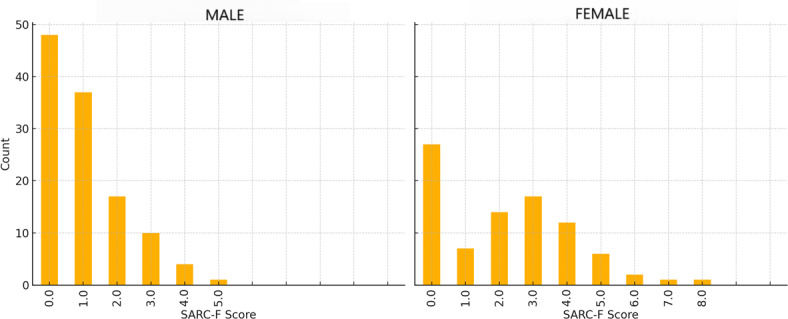
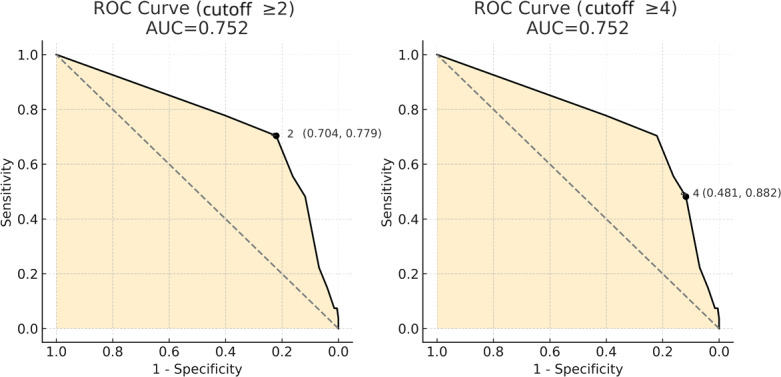
Results: Probable sarcopenia was present in 12% (n=24) of participants. The mean age (73.9, SD 6.2 years) and mean BMI (29.5, SD 5.8 kg/m²) did not differ significantly by sex; however, men showed a higher mean grip strength (36.3, SD 8.1 kg vs 22.4, SD 5.5 kg; P<.001) and lower mean SARC-F scores (0.9, SD 1.7 vs 1.9, SD 2.3; P<.001). A SARC-F cut point of ≥2 yielded an area under the curve of 0.77 (95% CI 0.67-0.88), with sensitivity of 0.78, specificity of 0.75, accuracy of 0.77, positive predictive value of 0.31, and negative predictive value of 0.96. The grip strength differed significantly between screen-positive and screen-negative groups at both the ≥2 and ≥4 thresholds (P<.001).
Conclusions: A SARC- F threshold of ≥2 is recommended as an optimal trade-off between sensitivity and specificity for identifying community-dwelling older adults with probable sarcopenia. This threshold is lower than the currently accepted recommendation of ≥4. Our findings promote the recommendations for early detection and treatment by medical professionals following the EWGSOP2 by improving the ability of clinicians to identify individuals with low muscle strength using this screening procedure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


