Abdulrahman Omar A Alali, Abdualaziz Fayez Alhumidi Alanazi, Mohammed Abdulaziz M Albarghash, Rakan Nasser Abdullah Alruweli, Mohammed Bader H Alanazi, Ibrahim Farhan B Alanazi, Turkey Saleh H Alrowaily, Rakan Khalid Marzouq Alanazi, Baraah AbuAlsel, Fadih Nada M Alenezi, Rashad Qasem Ali Othman, Manal S Fawzy
{"title":"Incidence of Gallstones in Patients with Obesity After Bariatric Surgery in Northern Saudi Arabia: A Cross-Sectional Study.","authors":"Abdulrahman Omar A Alali, Abdualaziz Fayez Alhumidi Alanazi, Mohammed Abdulaziz M Albarghash, Rakan Nasser Abdullah Alruweli, Mohammed Bader H Alanazi, Ibrahim Farhan B Alanazi, Turkey Saleh H Alrowaily, Rakan Khalid Marzouq Alanazi, Baraah AbuAlsel, Fadih Nada M Alenezi, Rashad Qasem Ali Othman, Manal S Fawzy","doi":"10.3390/clinpract15070115","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/objectives: </strong>Gallstone formation (cholelithiasis) is a common and important consequence following bariatric surgery, though regional data from the Northern Border Region are limited. This study aimed to investigate the incidence and risk factors of gallstones in this population, with the goal of optimizing postoperative treatment and reducing morbidity.</p><p><strong>Methods: </strong>We conducted a cross-sectional study using a non-probability convenience sampling technique to recruit 509 participants with varying degrees of obesity. Four hundred and ten study participants underwent bariatric surgery, of whom 73 were excluded for preoperative cholelithiasis and/or cholecystectomy. Data were collected through a self-administered, pre-validated questionnaire distributed via various social media platforms. These data included demographics, type/timing of surgery, pre/postoperative BMI, medical history, use of gallstone prophylaxis, and gallstone outcomes. Logistic regression analysis was used to identify independent predictors of gallstone formation.</p><p><strong>Results: </strong>Postoperative cholelithiasis developed in 60.8% of patients, most commonly within the first postoperative year, with risk peaking between 7 and 12 months after surgery. Rapid and substantial postoperative weight loss, as reflected in a lower current BMI and a transition to normal or overweight status within one year, was significantly associated with an increased incidence of gallstones. Female sex (OR: 2.62, 95% CI: 1.38-4.98, <i>p</i> = 0.003) and non-use of gallstone prevention medication (OR: 4.12, 95% CI: 1.34-12.64, <i>p</i> = 0.013) were independent predictors of gallstone formation. A longer time since surgery (OR: 0.76, 95% CI: 0.63-0.91, <i>p</i> = 0.004) and a lower current BMI (OR: 0.48, 95% CI: 0.28-0.83, <i>p</i> = 0.008) were associated with a reduced risk. Smoking status and comorbidities were not significantly related to the risk of gallstones.</p><p><strong>Conclusions: </strong>Gallstone formation after bariatric surgery in this population is influenced by female sex, rapid postoperative weight loss, and lack of prophylactic medication, while the type of surgical procedure does not significantly affect risk. Focused monitoring and preventive strategies, particularly in high-risk groups, are recommended to reduce gallstone-related complications following bariatric surgery.</p>","PeriodicalId":45306,"journal":{"name":"Clinics and Practice","volume":"15 7","pages":""},"PeriodicalIF":2.2000,"publicationDate":"2025-06-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12293454/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinics and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/clinpract15070115","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background/objectives: Gallstone formation (cholelithiasis) is a common and important consequence following bariatric surgery, though regional data from the Northern Border Region are limited. This study aimed to investigate the incidence and risk factors of gallstones in this population, with the goal of optimizing postoperative treatment and reducing morbidity.
Methods: We conducted a cross-sectional study using a non-probability convenience sampling technique to recruit 509 participants with varying degrees of obesity. Four hundred and ten study participants underwent bariatric surgery, of whom 73 were excluded for preoperative cholelithiasis and/or cholecystectomy. Data were collected through a self-administered, pre-validated questionnaire distributed via various social media platforms. These data included demographics, type/timing of surgery, pre/postoperative BMI, medical history, use of gallstone prophylaxis, and gallstone outcomes. Logistic regression analysis was used to identify independent predictors of gallstone formation.
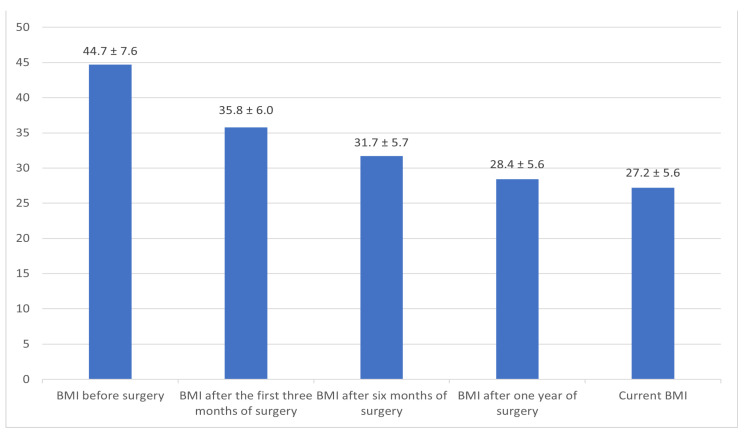
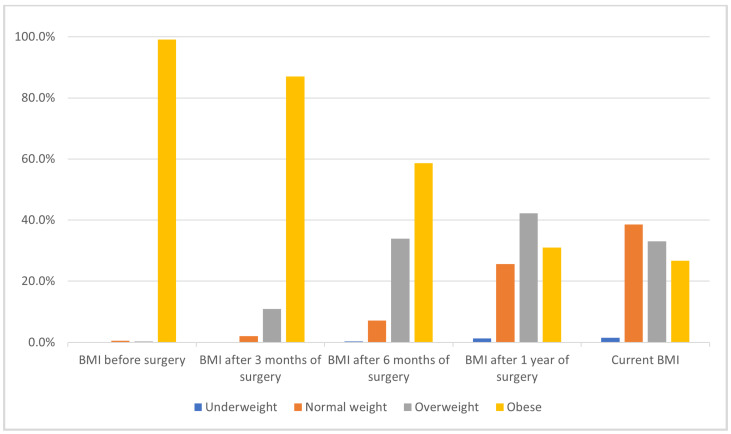
Results: Postoperative cholelithiasis developed in 60.8% of patients, most commonly within the first postoperative year, with risk peaking between 7 and 12 months after surgery. Rapid and substantial postoperative weight loss, as reflected in a lower current BMI and a transition to normal or overweight status within one year, was significantly associated with an increased incidence of gallstones. Female sex (OR: 2.62, 95% CI: 1.38-4.98, p = 0.003) and non-use of gallstone prevention medication (OR: 4.12, 95% CI: 1.34-12.64, p = 0.013) were independent predictors of gallstone formation. A longer time since surgery (OR: 0.76, 95% CI: 0.63-0.91, p = 0.004) and a lower current BMI (OR: 0.48, 95% CI: 0.28-0.83, p = 0.008) were associated with a reduced risk. Smoking status and comorbidities were not significantly related to the risk of gallstones.
Conclusions: Gallstone formation after bariatric surgery in this population is influenced by female sex, rapid postoperative weight loss, and lack of prophylactic medication, while the type of surgical procedure does not significantly affect risk. Focused monitoring and preventive strategies, particularly in high-risk groups, are recommended to reduce gallstone-related complications following bariatric surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


