Naonori Tashiro, Hiroki Nishiwaki, Takashi Ikeda, William M M Levack, Hisashi Noma, Noyuri Yamaji, Erika Ota, Takeshi Hasegawa
{"title":"Clinical utility of diaphragmatic ultrasound for mechanical ventilator liberation in adults: a systematic review and meta-analysis.","authors":"Naonori Tashiro, Hiroki Nishiwaki, Takashi Ikeda, William M M Levack, Hisashi Noma, Noyuri Yamaji, Erika Ota, Takeshi Hasegawa","doi":"10.1186/s40560-025-00811-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prolonged mechanical ventilation is associated with an increased incidence of complications and higher mortality rates. Therefore, it is crucial to wean patients from mechanical ventilation as soon as possible. Recently, diaphragmatic ultrasound has been used in this decision-making process. This systematic review evaluated the effectiveness of diaphragmatic ultrasound to improve ventilator liberation outcomes.</p><p><strong>Methods: </strong>We searched three databases - MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials. We included randomized control trials that compared the use of diaphragmatic ultrasound to standard care in adult patients on mechanical ventilation via tracheal intubation. We assessed risk of bias for included trials with the Cochrane Risk of Bias Tool and certainty of evidence using the Grading of Recommendations, Assessment, Development, and Evaluation tool. For dichotomous outcomes, we reported risk ratios (RRs) with 95% confidence intervals (CIs). For continuous outcomes, we reported mean differences (MD) with 95% CIs if all retrieved records provide data on the same scale. The primary outcome was incidence of reintubation within 48 h of extubation and the secondary outcomes included duration of mechanical ventilation, incidence of reintubation rate after 48 h, ICU length of stay, and adverse events.</p><p><strong>Results: </strong>We found five relevant randomized controlled trials involving a total of 508 participants on mechanical ventilation in ICU following respiratory failure or surgery. Three studies (268 participants) provided data on the incidence of reintubation within 48 h of extubation. Using diaphragmatic ultrasound to guide extubation decisions led to a significant reduction in the risk of reintubation within 48 h (RR 0.62, 95% CI 0.41 to 0.95, low certainty of evidence). No significant differences were found in the duration of mechanical ventilation (MD - 1.39 h, 95% CI - 17.5 to 14.71 h, three studies, 268 participants, very low certainty of evidence) or reintubation after 48 h (RR 0.38, 95% CI 0.11-1.29, two studies, 240 participants, moderate certainty of evidence). However, ICU length of stay was significantly reduced in the diaphragmatic ultrasound group (MD - 1.0 days, 95% CI - 1.74 to - 0.26 days, one study, 130 participants, low certainty of evidence).</p><p><strong>Conclusion: </strong>Using diaphragmatic ultrasound in addition to standard clinical criteria to guide decisions around ventilator use and liberation resulted in a reduced risk of reintubation within 48 h of extubation when compared to standard clinical criteria alone.</p><p><strong>Systematic review registration: </strong>This systematic review was registered with the Open Science Framework: https://osf.io/cn8xf .</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"13 1","pages":"40"},"PeriodicalIF":4.7000,"publicationDate":"2025-07-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12288223/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-025-00811-0","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Prolonged mechanical ventilation is associated with an increased incidence of complications and higher mortality rates. Therefore, it is crucial to wean patients from mechanical ventilation as soon as possible. Recently, diaphragmatic ultrasound has been used in this decision-making process. This systematic review evaluated the effectiveness of diaphragmatic ultrasound to improve ventilator liberation outcomes.
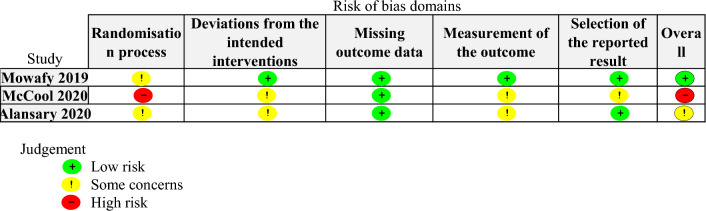
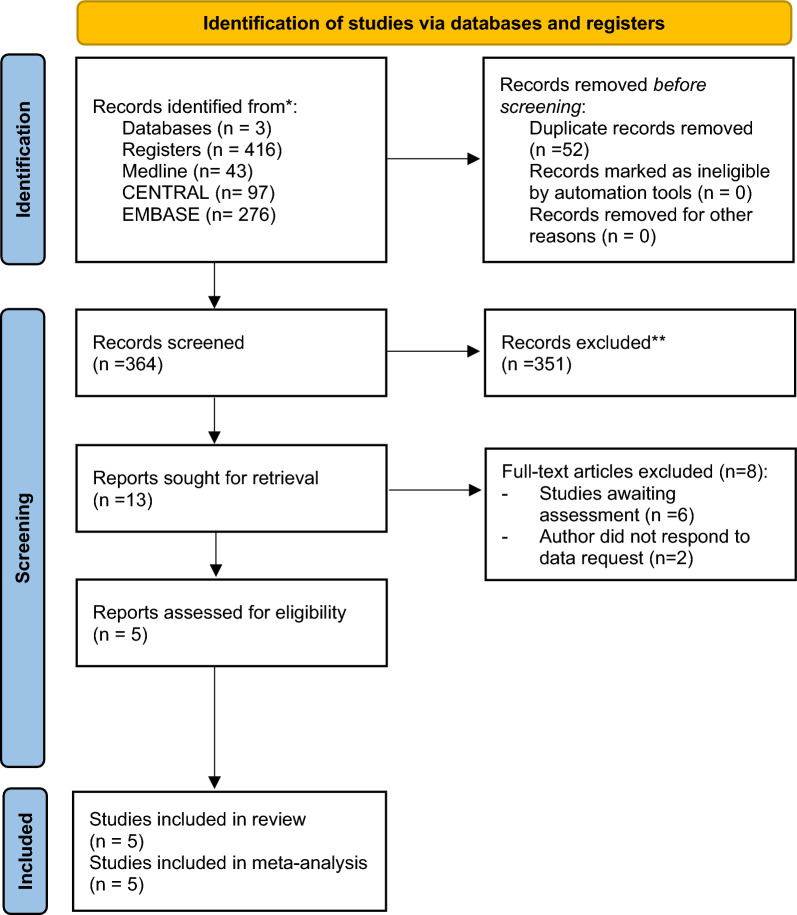
Methods: We searched three databases - MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials. We included randomized control trials that compared the use of diaphragmatic ultrasound to standard care in adult patients on mechanical ventilation via tracheal intubation. We assessed risk of bias for included trials with the Cochrane Risk of Bias Tool and certainty of evidence using the Grading of Recommendations, Assessment, Development, and Evaluation tool. For dichotomous outcomes, we reported risk ratios (RRs) with 95% confidence intervals (CIs). For continuous outcomes, we reported mean differences (MD) with 95% CIs if all retrieved records provide data on the same scale. The primary outcome was incidence of reintubation within 48 h of extubation and the secondary outcomes included duration of mechanical ventilation, incidence of reintubation rate after 48 h, ICU length of stay, and adverse events.
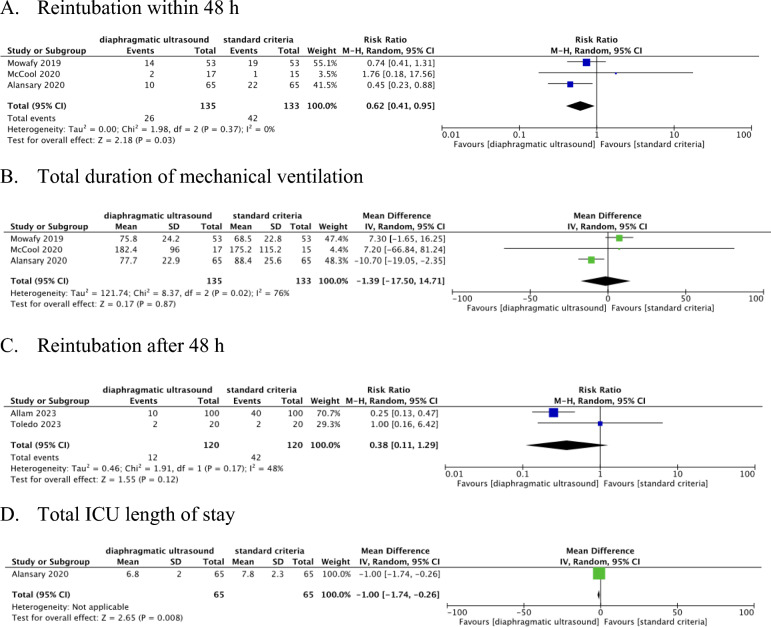
Results: We found five relevant randomized controlled trials involving a total of 508 participants on mechanical ventilation in ICU following respiratory failure or surgery. Three studies (268 participants) provided data on the incidence of reintubation within 48 h of extubation. Using diaphragmatic ultrasound to guide extubation decisions led to a significant reduction in the risk of reintubation within 48 h (RR 0.62, 95% CI 0.41 to 0.95, low certainty of evidence). No significant differences were found in the duration of mechanical ventilation (MD - 1.39 h, 95% CI - 17.5 to 14.71 h, three studies, 268 participants, very low certainty of evidence) or reintubation after 48 h (RR 0.38, 95% CI 0.11-1.29, two studies, 240 participants, moderate certainty of evidence). However, ICU length of stay was significantly reduced in the diaphragmatic ultrasound group (MD - 1.0 days, 95% CI - 1.74 to - 0.26 days, one study, 130 participants, low certainty of evidence).
Conclusion: Using diaphragmatic ultrasound in addition to standard clinical criteria to guide decisions around ventilator use and liberation resulted in a reduced risk of reintubation within 48 h of extubation when compared to standard clinical criteria alone.
Systematic review registration: This systematic review was registered with the Open Science Framework: https://osf.io/cn8xf .
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:



