Jorge Campos, Jose Luis Bas, Gonzalo Mariscal, Ibrahim Khalil, Mohammad Alzoubi, Paloma Bas, Teresa Bas
{"title":"Risk assessment of spinal surgery in chronic kidney disease and dialysis patients: a systematic review and meta-analysis of over 5 million cases.","authors":"Jorge Campos, Jose Luis Bas, Gonzalo Mariscal, Ibrahim Khalil, Mohammad Alzoubi, Paloma Bas, Teresa Bas","doi":"10.31616/asj.2024.0553","DOIUrl":null,"url":null,"abstract":"<p><p>The purpose of this study was to conduct a systematic review and meta-analysis of the outcomes of spinal surgery in patients with chronic kidney disease (CKD), including those undergoing dialysis. A comprehensive literature search was conducted following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines. Statistical analyses were performed using Review Manager software, utilizing mean differences (MD), odds ratios (OR), and random effects models to account for heterogeneity. Heterogeneity was assessed using the I2 statistic. The primary outcomes were operative time, estimated blood loss, need for blood transfusion, length of hospital stay, and the incidence of complications, including deep vein thrombosis (DVT), pulmonary embolism (PE), surgical site infection (SSI), reoperation, and in-hospital mortality. Twelve studies involving over 5 million patients were included, comparing outcomes in CKD and dialysis patients undergoing spinal surgery to those without CKD or dialysis, respectively. CKD patients experienced a significantly shorter operative time (MD, -12.63 minutes; 95% confidence interval [CI], -14.49 to -10.78) and longer hospital stays (MD, 1.51 days; 95% CI, 1.28-1.74), with moderate heterogeneity (I2=37%). Dialysis patients showed higher odds of developing DVT (OR, 6.45; 95% CI, 1.72-24.20), PE (OR, 6.48; 95% CI, 1.13-37.14), and in-hospital mortality (OR, 16.71; 95% CI, 6.23-44.85), with substantial heterogeneity among studies (I2>95%). Additionally, dialysis patients had significantly higher odds of requiring reoperation (OR, 7.04; 95% CI, 2.49-19.86) and longer hospital stays (MD, 5.89 days; 95% CI, 3.58-8.20). CKD and dialysis patients face higher risks following spine surgery compared to their counterparts with normal kidney function. Our study highlights the need for extra care and monitoring of kidney disease patients undergoing spine surgery.</p>","PeriodicalId":8555,"journal":{"name":"Asian Spine Journal","volume":" ","pages":"652-670"},"PeriodicalIF":2.7000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400105/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asian Spine Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31616/asj.2024.0553","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/25 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
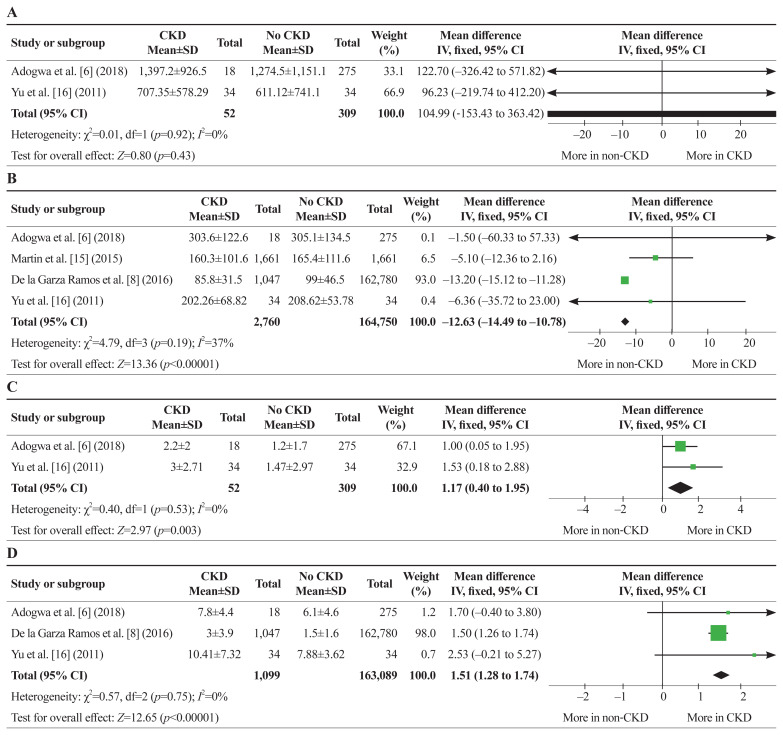
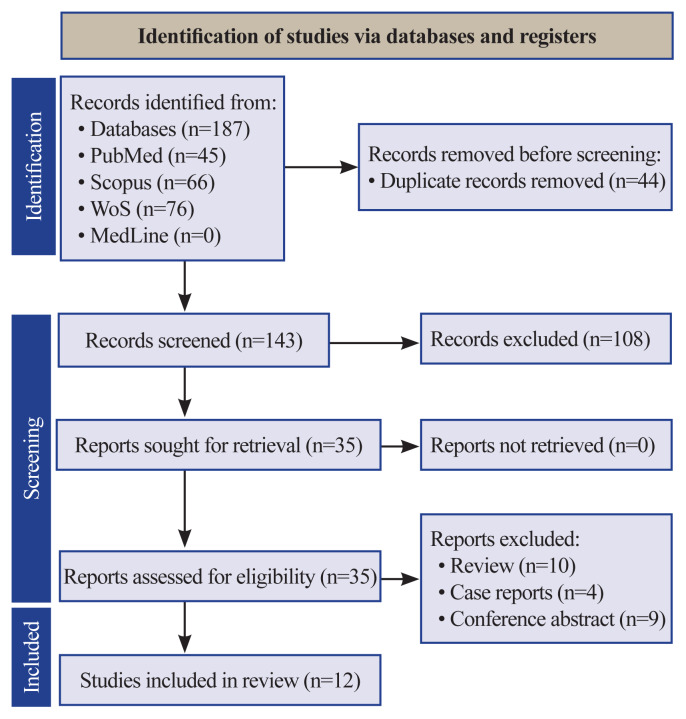
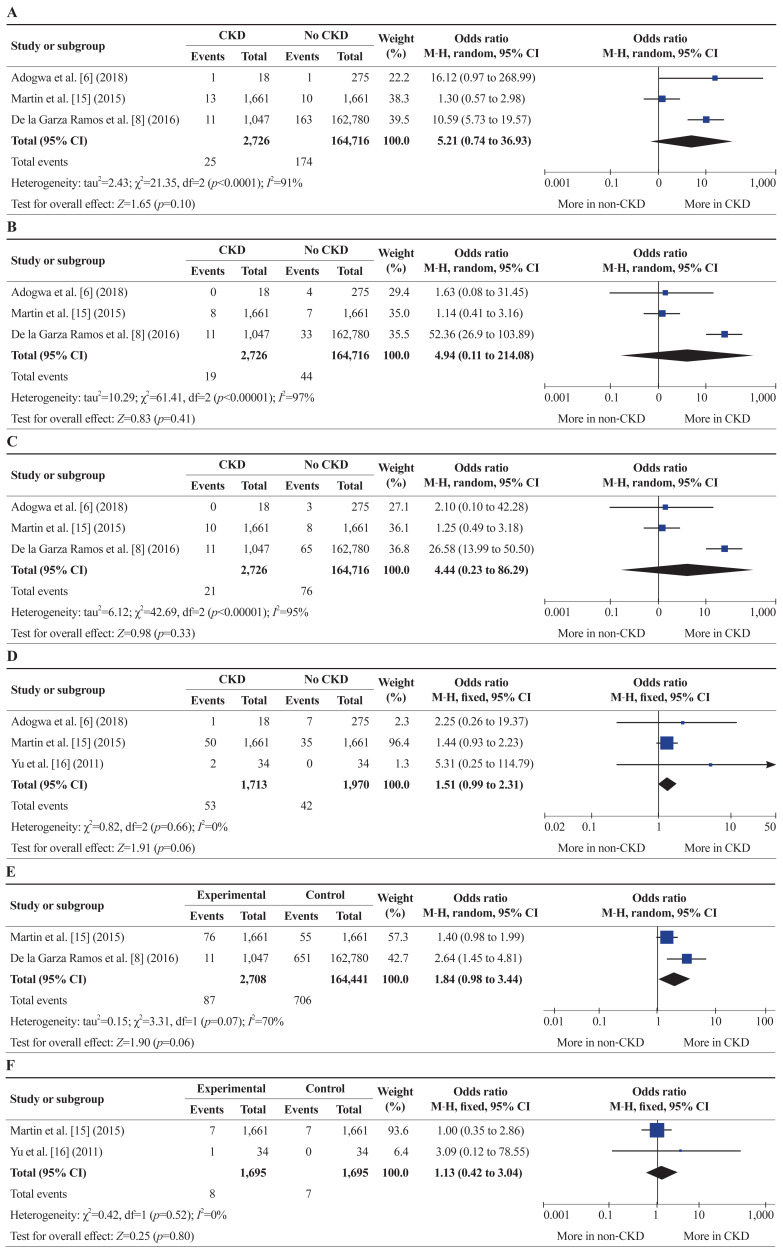
The purpose of this study was to conduct a systematic review and meta-analysis of the outcomes of spinal surgery in patients with chronic kidney disease (CKD), including those undergoing dialysis. A comprehensive literature search was conducted following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines. Statistical analyses were performed using Review Manager software, utilizing mean differences (MD), odds ratios (OR), and random effects models to account for heterogeneity. Heterogeneity was assessed using the I2 statistic. The primary outcomes were operative time, estimated blood loss, need for blood transfusion, length of hospital stay, and the incidence of complications, including deep vein thrombosis (DVT), pulmonary embolism (PE), surgical site infection (SSI), reoperation, and in-hospital mortality. Twelve studies involving over 5 million patients were included, comparing outcomes in CKD and dialysis patients undergoing spinal surgery to those without CKD or dialysis, respectively. CKD patients experienced a significantly shorter operative time (MD, -12.63 minutes; 95% confidence interval [CI], -14.49 to -10.78) and longer hospital stays (MD, 1.51 days; 95% CI, 1.28-1.74), with moderate heterogeneity (I2=37%). Dialysis patients showed higher odds of developing DVT (OR, 6.45; 95% CI, 1.72-24.20), PE (OR, 6.48; 95% CI, 1.13-37.14), and in-hospital mortality (OR, 16.71; 95% CI, 6.23-44.85), with substantial heterogeneity among studies (I2>95%). Additionally, dialysis patients had significantly higher odds of requiring reoperation (OR, 7.04; 95% CI, 2.49-19.86) and longer hospital stays (MD, 5.89 days; 95% CI, 3.58-8.20). CKD and dialysis patients face higher risks following spine surgery compared to their counterparts with normal kidney function. Our study highlights the need for extra care and monitoring of kidney disease patients undergoing spine surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


