{"title":"Conditions Associated With the Onset of Cancer After Heart Transplant: Longitudinal Study in 335 Recipients","authors":"Fabian Patauner, Filomena Boccia, Silvia Masini, Giuliana Autiero, Raffaella Gallo, Lorenzo Bertolino, Irene Mattucci, Daniela Pinto, Roberto Andini, Cristiano Amarelli, Rosa Zampino, Emanuele Durante-Mangoni","doi":"10.1111/ctr.70243","DOIUrl":null,"url":null,"abstract":"<p>Cancer is among the major causes of death after heart transplant (HTx). Risk factors for cancer occurrence in this setting are not well established. This was a retrospective observational study of patients who underwent HTx between 2006 and 2019 and were followed up until May 2024. Clinical variables possibly associated with cancer were assessed with univariable and multivariable analyses. Survival analysis was carried out drawing Kaplan Meier curves and a Cox regression with time-varying covariates were performed to overcome the immortal-time-bias. Three-hundred-thirty-five HTx recipients were included, of whom 42 (12.5%) developed cancer after a median of 6.3 years. In univariable analysis, older age at HTx, smoking history, alcohol use, male sex, ischemic heart disease before HTx, use of cyclosporine rather than tacrolimus, and increased length of follow-up were associated with cancer. Upon multivariable analysis, ischemic heart disease (OR 2.70 [1.19–6.11], <i>p</i> = 0.017) and length of follow-up (OR 1.02 [1.00–1.04], <i>p</i> = 0.007) were independently associated with cancer occurrence. Cox regression revealed a higher risk of mortality among patients with cancer (HR 3.400, [2.026–5.709], <i>p</i> < 0.001). HTx recipients with prior ischemic cardiomyopathy and a longer survival time after transplant show a higher risk of developing cancer. Cancer significantly impairs post-transplant survival.</p>","PeriodicalId":10467,"journal":{"name":"Clinical Transplantation","volume":"39 8","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2025-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ctr.70243","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Transplantation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ctr.70243","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
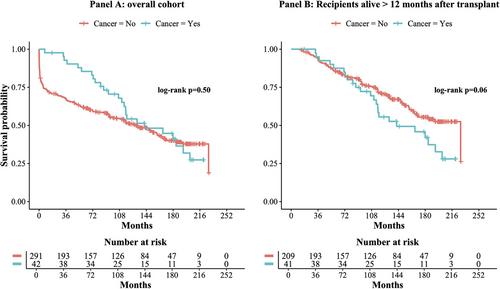
Cancer is among the major causes of death after heart transplant (HTx). Risk factors for cancer occurrence in this setting are not well established. This was a retrospective observational study of patients who underwent HTx between 2006 and 2019 and were followed up until May 2024. Clinical variables possibly associated with cancer were assessed with univariable and multivariable analyses. Survival analysis was carried out drawing Kaplan Meier curves and a Cox regression with time-varying covariates were performed to overcome the immortal-time-bias. Three-hundred-thirty-five HTx recipients were included, of whom 42 (12.5%) developed cancer after a median of 6.3 years. In univariable analysis, older age at HTx, smoking history, alcohol use, male sex, ischemic heart disease before HTx, use of cyclosporine rather than tacrolimus, and increased length of follow-up were associated with cancer. Upon multivariable analysis, ischemic heart disease (OR 2.70 [1.19–6.11], p = 0.017) and length of follow-up (OR 1.02 [1.00–1.04], p = 0.007) were independently associated with cancer occurrence. Cox regression revealed a higher risk of mortality among patients with cancer (HR 3.400, [2.026–5.709], p < 0.001). HTx recipients with prior ischemic cardiomyopathy and a longer survival time after transplant show a higher risk of developing cancer. Cancer significantly impairs post-transplant survival.
期刊介绍:
Clinical Transplantation: The Journal of Clinical and Translational Research aims to serve as a channel of rapid communication for all those involved in the care of patients who require, or have had, organ or tissue transplants, including: kidney, intestine, liver, pancreas, islets, heart, heart valves, lung, bone marrow, cornea, skin, bone, and cartilage, viable or stored.
Published monthly, Clinical Transplantation’s scope is focused on the complete spectrum of present transplant therapies, as well as also those that are experimental or may become possible in future. Topics include:
Immunology and immunosuppression;
Patient preparation;
Social, ethical, and psychological issues;
Complications, short- and long-term results;
Artificial organs;
Donation and preservation of organ and tissue;
Translational studies;
Advances in tissue typing;
Updates on transplant pathology;.
Clinical and translational studies are particularly welcome, as well as focused reviews. Full-length papers and short communications are invited. Clinical reviews are encouraged, as well as seminal papers in basic science which might lead to immediate clinical application. Prominence is regularly given to the results of cooperative surveys conducted by the organ and tissue transplant registries.
Clinical Transplantation: The Journal of Clinical and Translational Research is essential reading for clinicians and researchers in the diverse field of transplantation: surgeons; clinical immunologists; cryobiologists; hematologists; gastroenterologists; hepatologists; pulmonologists; nephrologists; cardiologists; and endocrinologists. It will also be of interest to sociologists, psychologists, research workers, and to all health professionals whose combined efforts will improve the prognosis of transplant recipients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


