Georgios Farantos, Athanasios Pitis, Maria Diamantopoulou, Fotini Tzavella
{"title":"Measuring Health Inequalities Using the Robin Hood Index: A Systematic Review with Meta-Analysis.","authors":"Georgios Farantos, Athanasios Pitis, Maria Diamantopoulou, Fotini Tzavella","doi":"10.3390/epidemiologia6030035","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background/Objectives:</b> Although the Robin Hood Index (RHI) is increasingly used to quantify geographic health inequality and guide resource redistribution, empirical evidence on whether higher physician density reduces RHI-measured inequality remains limited. This study systematically reviews and meta-analyzes RHI-based research to assess the association between physician distribution and health inequalities. <b>Methods:</b> We conducted a systematic review and meta-analysis of studies using the RHI to evaluate health inequalities, without restrictions on country or publication date. Following PRISMA 2020 guidelines and registered in PROSPERO (CRD42024496486), we searched PubMed, Scopus, and OpenGrey literature, extracted data on physician density and RHI outcomes, and conducted a meta-analysis. Odds ratios (ORs), ln(OR), and 95% confidence intervals (CIs) were calculated, and risk of bias was assessed using the Robvis tool. <b>Results:</b> Seventeen studies covering 720 regions and 1.07 billion individuals were included. Three clusters emerged: physician redistribution (10 studies), poverty-mortality associations (six studies), and systematic reviews (one study). Physician redistribution was strongly associated with increased inequality and policy attention (r = 0.73; <i>p</i> = 0.0038). Meta-analysis of eight redistribution studies yielded a pooled OR of 1.24 (95% CI: 0.54-2.86), consistent in sensitivity analysis (OR = 1.26; 95% CI: 0.56-2.89). Poverty-mortality studies also showed a correlation with the number of variables considered (r = 0.59; <i>p</i> = 0.022). <b>Conclusions:</b> A greater physician supply is associated with increased health inequalities, with statistical support but limited certainty. Methodological heterogeneity in RHI-based studies constrains comparability. Standardized methodologies and broader analytic models are needed to inform research and guide health policy.</p>","PeriodicalId":72944,"journal":{"name":"Epidemiolgia (Basel, Switzerland)","volume":"6 3","pages":""},"PeriodicalIF":2.2000,"publicationDate":"2025-07-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12285989/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Epidemiolgia (Basel, Switzerland)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/epidemiologia6030035","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
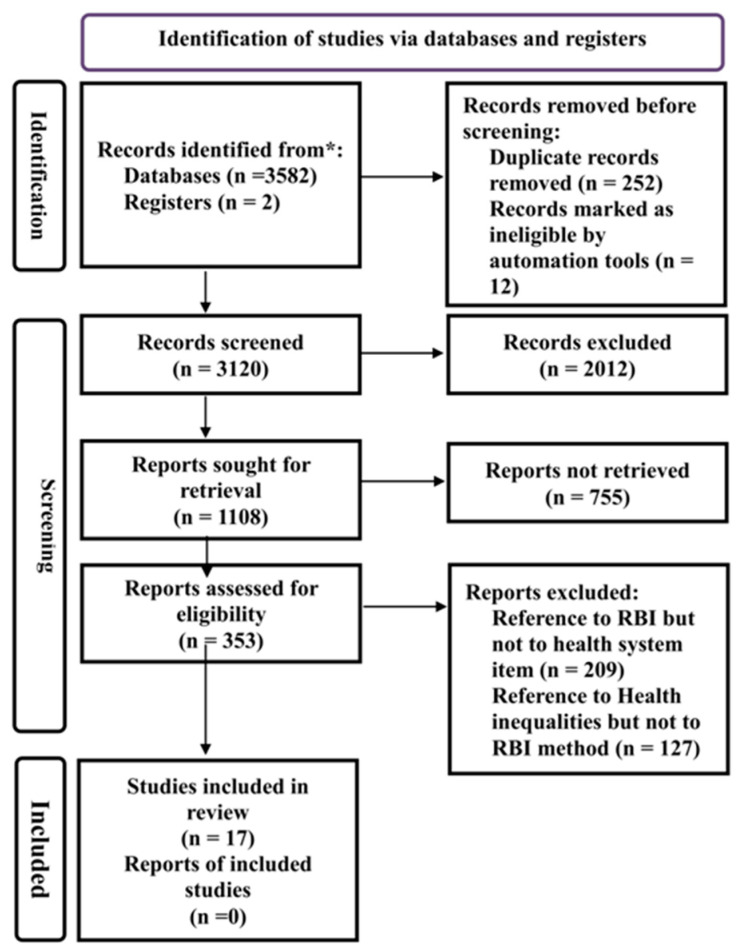
Background/Objectives: Although the Robin Hood Index (RHI) is increasingly used to quantify geographic health inequality and guide resource redistribution, empirical evidence on whether higher physician density reduces RHI-measured inequality remains limited. This study systematically reviews and meta-analyzes RHI-based research to assess the association between physician distribution and health inequalities. Methods: We conducted a systematic review and meta-analysis of studies using the RHI to evaluate health inequalities, without restrictions on country or publication date. Following PRISMA 2020 guidelines and registered in PROSPERO (CRD42024496486), we searched PubMed, Scopus, and OpenGrey literature, extracted data on physician density and RHI outcomes, and conducted a meta-analysis. Odds ratios (ORs), ln(OR), and 95% confidence intervals (CIs) were calculated, and risk of bias was assessed using the Robvis tool. Results: Seventeen studies covering 720 regions and 1.07 billion individuals were included. Three clusters emerged: physician redistribution (10 studies), poverty-mortality associations (six studies), and systematic reviews (one study). Physician redistribution was strongly associated with increased inequality and policy attention (r = 0.73; p = 0.0038). Meta-analysis of eight redistribution studies yielded a pooled OR of 1.24 (95% CI: 0.54-2.86), consistent in sensitivity analysis (OR = 1.26; 95% CI: 0.56-2.89). Poverty-mortality studies also showed a correlation with the number of variables considered (r = 0.59; p = 0.022). Conclusions: A greater physician supply is associated with increased health inequalities, with statistical support but limited certainty. Methodological heterogeneity in RHI-based studies constrains comparability. Standardized methodologies and broader analytic models are needed to inform research and guide health policy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


