Markus Koster, Katrin Ledergerber, Michael Brändle
{"title":"'Un-thirsty' hypernatremia.","authors":"Markus Koster, Katrin Ledergerber, Michael Brändle","doi":"10.1530/EDM-25-0008","DOIUrl":null,"url":null,"abstract":"<p><strong>Summary: </strong>A 38-year-old man was admitted because of transient somnolence. Five weeks previously, he had suffered a subarachnoid hemorrhage from a ruptured aneurysm of the anterior communicating artery (ACOM), which was treated by craniotomy and clipping. He had recovered well, although loss of short-term memory and a forehead paresis on the side of craniotomy persisted. Clinical examination on admission showed no new neurological deficits. Cerebral computed tomography with angiography revealed no bleeding or infarction and correctly positioned clips. Laboratory examination showed severe hypernatremia (179 mmol/L). The patient was admitted to the intensive care unit (ICU) and treated with oral fluids and 5% glucose intravenously. Remarkably, he denied being thirsty and had to be encouraged to drink. Urine osmolality quickly fell to 294 mOsm/kg, polyuria of up to 400 mL/h was measured, and serum sodium remained elevated. Therefore, diabetes insipidus (DI) was obvious. After application of desmopressin acetate, urine output dropped to around 50 mL/h, confirming central DI or vasopressin deficiency (VD). Desmopressin acetate dose and volume management were continuously adjusted to blood sodium to restore euvolemia. Drinking volume needed to be supervised because of persistent lack of thirst and amnesia of being told to drink. Adipsic VD (aAVP-D) is a rare syndrome characterized by the combination of VD and loss of thirst in response to hypernatremia. It usually occurs within days after cell damage of osmoreceptors, for example after disruption of blood supply as in clipping of an ACOM aneurysm. Management includes titrated desmopressin acetate replacement, fixed water intake, weight monitoring, patient education and sodium monitoring.</p><p><strong>Learning points: </strong>Adipsic vasopressin deficiency (aAVP-D) is a rare form of vasopressin deficiency (VD) characterized by additional loss of thirst in response to hypernatremia due to impaired function of periventricular osmoreceptors. Bleeding from ACOM aneurysm and, possibly, therefore the performed frontal craniectomy with aneurysm clipping are the most frequent causes of aAVP-D. Other causes include craniopharyngioma, head trauma, germinoma or neurosarcoidosis. Management of aAVP-D includes replacement of titrated desmopressin acetate, fixed water intake, daily weight tracking, good patient education and regular sodium monitoring.</p>","PeriodicalId":37467,"journal":{"name":"Endocrinology, Diabetes and Metabolism Case Reports","volume":"2025 3","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-07-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12291485/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrinology, Diabetes and Metabolism Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EDM-25-0008","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"Print","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
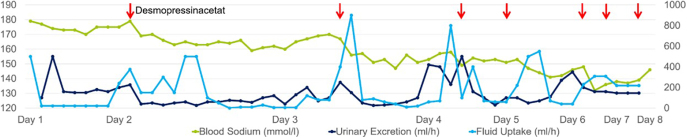
Summary: A 38-year-old man was admitted because of transient somnolence. Five weeks previously, he had suffered a subarachnoid hemorrhage from a ruptured aneurysm of the anterior communicating artery (ACOM), which was treated by craniotomy and clipping. He had recovered well, although loss of short-term memory and a forehead paresis on the side of craniotomy persisted. Clinical examination on admission showed no new neurological deficits. Cerebral computed tomography with angiography revealed no bleeding or infarction and correctly positioned clips. Laboratory examination showed severe hypernatremia (179 mmol/L). The patient was admitted to the intensive care unit (ICU) and treated with oral fluids and 5% glucose intravenously. Remarkably, he denied being thirsty and had to be encouraged to drink. Urine osmolality quickly fell to 294 mOsm/kg, polyuria of up to 400 mL/h was measured, and serum sodium remained elevated. Therefore, diabetes insipidus (DI) was obvious. After application of desmopressin acetate, urine output dropped to around 50 mL/h, confirming central DI or vasopressin deficiency (VD). Desmopressin acetate dose and volume management were continuously adjusted to blood sodium to restore euvolemia. Drinking volume needed to be supervised because of persistent lack of thirst and amnesia of being told to drink. Adipsic VD (aAVP-D) is a rare syndrome characterized by the combination of VD and loss of thirst in response to hypernatremia. It usually occurs within days after cell damage of osmoreceptors, for example after disruption of blood supply as in clipping of an ACOM aneurysm. Management includes titrated desmopressin acetate replacement, fixed water intake, weight monitoring, patient education and sodium monitoring.
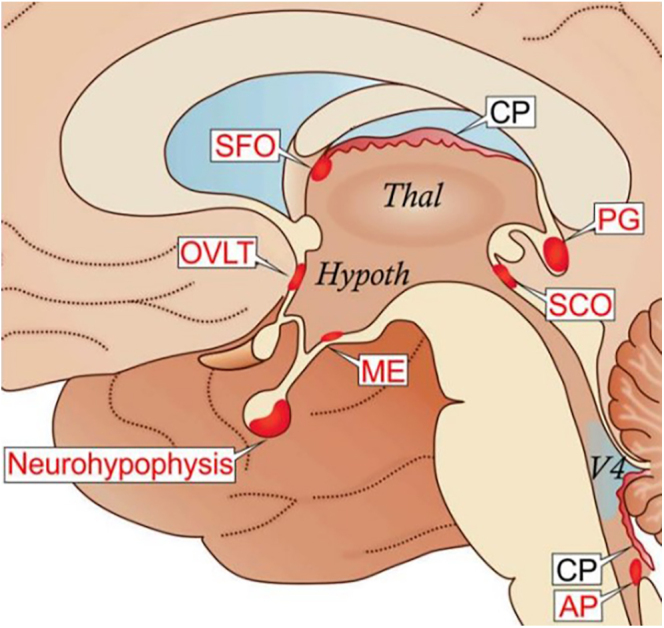
Learning points: Adipsic vasopressin deficiency (aAVP-D) is a rare form of vasopressin deficiency (VD) characterized by additional loss of thirst in response to hypernatremia due to impaired function of periventricular osmoreceptors. Bleeding from ACOM aneurysm and, possibly, therefore the performed frontal craniectomy with aneurysm clipping are the most frequent causes of aAVP-D. Other causes include craniopharyngioma, head trauma, germinoma or neurosarcoidosis. Management of aAVP-D includes replacement of titrated desmopressin acetate, fixed water intake, daily weight tracking, good patient education and regular sodium monitoring.
期刊介绍:
Endocrinology, Diabetes & Metabolism Case Reports publishes case reports on common and rare conditions in all areas of clinical endocrinology, diabetes and metabolism. Articles should include clear learning points which readers can use to inform medical education or clinical practice. The types of cases of interest to Endocrinology, Diabetes & Metabolism Case Reports include: -Insight into disease pathogenesis or mechanism of therapy - Novel diagnostic procedure - Novel treatment - Unique/unexpected symptoms or presentations of a disease - New disease or syndrome: presentations/diagnosis/management - Unusual effects of medical treatment - Error in diagnosis/pitfalls and caveats


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


