Fatima Iqbal, Daniel Lim, Ruby Chang, Akhil Gupta, Jeff Ahn, Nimalie Perera
{"title":"Severe hypertriglyceridaemia with length-related small fibre sensory neuropathy as a complication of previous gestational diabetes mellitus.","authors":"Fatima Iqbal, Daniel Lim, Ruby Chang, Akhil Gupta, Jeff Ahn, Nimalie Perera","doi":"10.1530/EDM-25-0060","DOIUrl":null,"url":null,"abstract":"<p><strong>Summary: </strong>Gestational diabetes mellitus (GDM) is a known risk factor for dyslipidaemias. Insulin resistance and the associated dyslipidaemia, particularly hypertriglyceridaemia, have been less frequently linked to peripheral nerve dysfunction, including small fibre sensory neuropathy. The relationship between metabolic disturbances, such as hypertriglyceridaemia, and neuropathy warrants further exploration and has gained increasing recognition in recent studies. This case highlights the potential neurological consequences of lipid abnormalities in women with a history of GDM. A 38-year-old woman presented to an endocrinologist with a 4-week history of paraesthesias and incidental findings of significantly elevated triglycerides (78.4 mmol/L) and total cholesterol (14.7 mmol/L). Initially, numbness began in her left first toe, spreading to other toes on the left foot, and then to the right foot, accompanied by hyperalgesia in fifth fingers bilaterally. She had no history of trauma or back injuries. Her medical history included insulin-dependent GDM and HELLP syndrome 4 years prior, endometriosis, and adenomyosis. With persistently high lipid levels (cholesterol: 12.1 mmol/L; triglycerides: 18.5 mmol/L), she was admitted to ICU for urgent lipid-lowering treatment but experienced hypoglycaemia on an insulin-dextrose infusion. Repeat triglycerides the next day were 13.1 mmol/L. A neurologist diagnosed her with small fibre sensory neuropathy secondary to hypertriglyceridaemia. Treatment with fenofibrate, high-dose fish oil, and a low-fat, low-carbohydrate diet was initiated with outpatient endocrinologist follow-up. Hypertriglyceridaemia is a significant health concern, potentially leading to severe complications such as peripheral neuropathy. Early intervention to optimise lipid levels is essential to prevent adverse outcomes.</p><p><strong>Learning points: </strong>GDM is known to be a risk factor for dyslipidaemias. Hypertriglyceridaemia can contribute to small fibre sensory neuropathy via mechanisms including microvascular ischaemia, oxidative stress, and inflammation affecting peripheral nerves. Diagnosis requires clinical correlation with lipid profiles and neurological findings, and exclusion of other causes through targeted investigations such as nerve conduction studies and autoimmune screening. Early recognition of hypertriglyceridaemia is essential to prevent complications such as neuropathy. Acute management may involve insulin-dextrose infusion in cases of severe elevation, while long-term treatment includes fibrates, omega-3 fatty acids, and dietary modifications.</p>","PeriodicalId":37467,"journal":{"name":"Endocrinology, Diabetes and Metabolism Case Reports","volume":"2025 3","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-07-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12285574/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrinology, Diabetes and Metabolism Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EDM-25-0060","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"Print","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
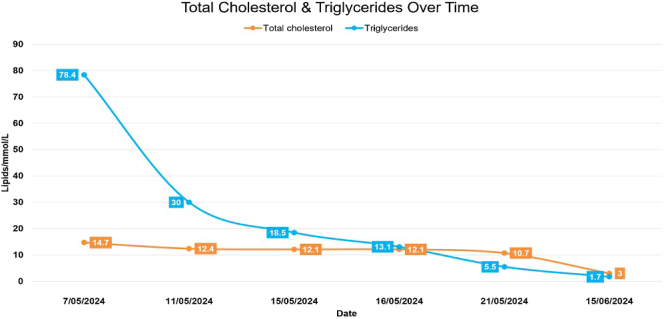
Summary: Gestational diabetes mellitus (GDM) is a known risk factor for dyslipidaemias. Insulin resistance and the associated dyslipidaemia, particularly hypertriglyceridaemia, have been less frequently linked to peripheral nerve dysfunction, including small fibre sensory neuropathy. The relationship between metabolic disturbances, such as hypertriglyceridaemia, and neuropathy warrants further exploration and has gained increasing recognition in recent studies. This case highlights the potential neurological consequences of lipid abnormalities in women with a history of GDM. A 38-year-old woman presented to an endocrinologist with a 4-week history of paraesthesias and incidental findings of significantly elevated triglycerides (78.4 mmol/L) and total cholesterol (14.7 mmol/L). Initially, numbness began in her left first toe, spreading to other toes on the left foot, and then to the right foot, accompanied by hyperalgesia in fifth fingers bilaterally. She had no history of trauma or back injuries. Her medical history included insulin-dependent GDM and HELLP syndrome 4 years prior, endometriosis, and adenomyosis. With persistently high lipid levels (cholesterol: 12.1 mmol/L; triglycerides: 18.5 mmol/L), she was admitted to ICU for urgent lipid-lowering treatment but experienced hypoglycaemia on an insulin-dextrose infusion. Repeat triglycerides the next day were 13.1 mmol/L. A neurologist diagnosed her with small fibre sensory neuropathy secondary to hypertriglyceridaemia. Treatment with fenofibrate, high-dose fish oil, and a low-fat, low-carbohydrate diet was initiated with outpatient endocrinologist follow-up. Hypertriglyceridaemia is a significant health concern, potentially leading to severe complications such as peripheral neuropathy. Early intervention to optimise lipid levels is essential to prevent adverse outcomes.
Learning points: GDM is known to be a risk factor for dyslipidaemias. Hypertriglyceridaemia can contribute to small fibre sensory neuropathy via mechanisms including microvascular ischaemia, oxidative stress, and inflammation affecting peripheral nerves. Diagnosis requires clinical correlation with lipid profiles and neurological findings, and exclusion of other causes through targeted investigations such as nerve conduction studies and autoimmune screening. Early recognition of hypertriglyceridaemia is essential to prevent complications such as neuropathy. Acute management may involve insulin-dextrose infusion in cases of severe elevation, while long-term treatment includes fibrates, omega-3 fatty acids, and dietary modifications.
期刊介绍:
Endocrinology, Diabetes & Metabolism Case Reports publishes case reports on common and rare conditions in all areas of clinical endocrinology, diabetes and metabolism. Articles should include clear learning points which readers can use to inform medical education or clinical practice. The types of cases of interest to Endocrinology, Diabetes & Metabolism Case Reports include: -Insight into disease pathogenesis or mechanism of therapy - Novel diagnostic procedure - Novel treatment - Unique/unexpected symptoms or presentations of a disease - New disease or syndrome: presentations/diagnosis/management - Unusual effects of medical treatment - Error in diagnosis/pitfalls and caveats



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


