Isuru Gamage, Emma Boehm, Gaurav Ghosh, Grace Kong, Michael Michael, HuiLi Wong, Oliver Piercey, Nirupa Sachithanandan
{"title":"Unmasking insulinoma following commencement of somatostatin analogues in malignant neuroendocrine tumours.","authors":"Isuru Gamage, Emma Boehm, Gaurav Ghosh, Grace Kong, Michael Michael, HuiLi Wong, Oliver Piercey, Nirupa Sachithanandan","doi":"10.1530/EO-25-0005","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Somatostatin analogues (SSA) are used in the management of patients with metastatic gastroenteropancreatic neuroendocrine tumours (GEP-NET) to control hormone secretion and tumour growth. SSA can paradoxically worsen or unmask hypoglycaemia in patients with insulinoma by inhibiting counter-regulatory hormones such as glucagon and growth hormone.</p><p><strong>Design and methods: </strong>We present two cases of SSA use in patients with initially presumed non-functioning GEP-NET unmasking insulinoma. We review the use of SSA in GEP-NET and the management of refractory hypoglycaemia in metastatic insulinoma.</p><p><strong>Results: </strong>A 62-year-old female with metastatic grade 2 GEP-NET was commenced on monthly lanreotide 10 weeks after diagnosis. She presented 1 week following the second dose with refractory hypoglycaemia and inappropriate hyperinsulinism, requiring inpatient dextrose infusion. SSA was stopped; however, she remained dextrose dependent despite the addition of diazoxide and dexamethasone. Peptide receptor radionuclide therapy (PRRT) with <sup>177</sup>Lu-DOTA-Octreotate was given, resulting in resolution of hypoglycaemia after two cycles. The second case is a 57-year-old female with metastatic grade 2 GEP-NET. Four months post commencement of lanreotide, she presented with radiological disease progression and symptomatic hypoglycaemia. A 72 h fast confirmed hyperinsulinaemic hypoglycaemia. SSA was stopped. A trial of diazoxide was not tolerated, and a prednisolone trial was ineffective. The patient underwent inpatient PRRT with euglycaemia achieved shortly afterwards.</p><p><strong>Conclusions: </strong>SSA can unmask hypoglycaemia secondary to insulinoma. Detection of new-onset hypoglycaemia requires careful clinical vigilance when commencing SSA in patients with GEP-NET initially presumed to be non-functional. Hypoglycaemia from metastatic insulinoma requires multidisciplinary management incorporating nutritional, medical and oncologic therapy. PRRT can be effective in managing refractory hypoglycaemia.</p><p><strong>Learning points: </strong>SSA use can unmask insulinoma in a NET presumed to be non-functional.SSA can paradoxically worsen hypoglycaemia in insulinoma due to suppression of counter-regulatory hormones.There are currently no biomarkers in routine clinical use to predict which patients will experience a worsening of hypoglycaemia after SSA initiation. Detection of new-onset hypoglycaemia requires clinical vigilance and education of patients to report symptoms early to enable prompt investigation and management.Symptomatic hypoglycaemia in metastatic insulinoma is challenging to manage and requires a multidisciplinary approach considering diet, medical therapy and urgent initiation or escalation of oncologic therapy.PRRT is a safe and effective strategy to achieve hormonal and oncologic control in metastatic insulinoma. Caution should be practised regarding flare of insulin release, and inpatient administration with expert endocrinology, nuclear medicine and oncology input should be considered.</p>","PeriodicalId":72907,"journal":{"name":"Endocrine oncology (Bristol, England)","volume":"5 1","pages":"e250005"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12281627/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrine oncology (Bristol, England)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EO-25-0005","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Somatostatin analogues (SSA) are used in the management of patients with metastatic gastroenteropancreatic neuroendocrine tumours (GEP-NET) to control hormone secretion and tumour growth. SSA can paradoxically worsen or unmask hypoglycaemia in patients with insulinoma by inhibiting counter-regulatory hormones such as glucagon and growth hormone.
Design and methods: We present two cases of SSA use in patients with initially presumed non-functioning GEP-NET unmasking insulinoma. We review the use of SSA in GEP-NET and the management of refractory hypoglycaemia in metastatic insulinoma.
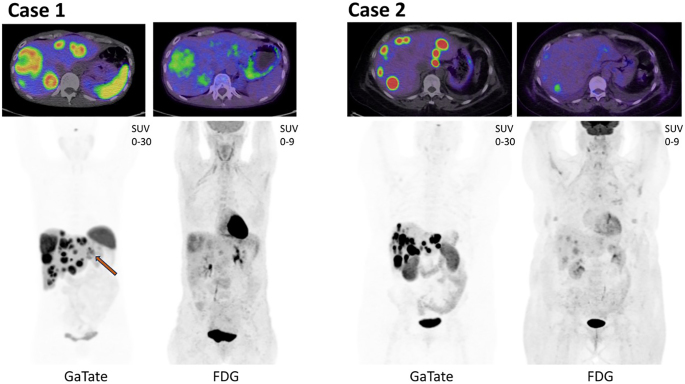
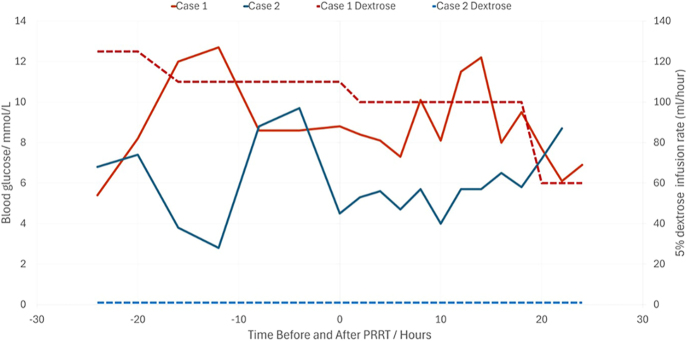
Results: A 62-year-old female with metastatic grade 2 GEP-NET was commenced on monthly lanreotide 10 weeks after diagnosis. She presented 1 week following the second dose with refractory hypoglycaemia and inappropriate hyperinsulinism, requiring inpatient dextrose infusion. SSA was stopped; however, she remained dextrose dependent despite the addition of diazoxide and dexamethasone. Peptide receptor radionuclide therapy (PRRT) with 177Lu-DOTA-Octreotate was given, resulting in resolution of hypoglycaemia after two cycles. The second case is a 57-year-old female with metastatic grade 2 GEP-NET. Four months post commencement of lanreotide, she presented with radiological disease progression and symptomatic hypoglycaemia. A 72 h fast confirmed hyperinsulinaemic hypoglycaemia. SSA was stopped. A trial of diazoxide was not tolerated, and a prednisolone trial was ineffective. The patient underwent inpatient PRRT with euglycaemia achieved shortly afterwards.
Conclusions: SSA can unmask hypoglycaemia secondary to insulinoma. Detection of new-onset hypoglycaemia requires careful clinical vigilance when commencing SSA in patients with GEP-NET initially presumed to be non-functional. Hypoglycaemia from metastatic insulinoma requires multidisciplinary management incorporating nutritional, medical and oncologic therapy. PRRT can be effective in managing refractory hypoglycaemia.
Learning points: SSA use can unmask insulinoma in a NET presumed to be non-functional.SSA can paradoxically worsen hypoglycaemia in insulinoma due to suppression of counter-regulatory hormones.There are currently no biomarkers in routine clinical use to predict which patients will experience a worsening of hypoglycaemia after SSA initiation. Detection of new-onset hypoglycaemia requires clinical vigilance and education of patients to report symptoms early to enable prompt investigation and management.Symptomatic hypoglycaemia in metastatic insulinoma is challenging to manage and requires a multidisciplinary approach considering diet, medical therapy and urgent initiation or escalation of oncologic therapy.PRRT is a safe and effective strategy to achieve hormonal and oncologic control in metastatic insulinoma. Caution should be practised regarding flare of insulin release, and inpatient administration with expert endocrinology, nuclear medicine and oncology input should be considered.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


