Patrick Leo, Behtash G Nezami, Mahmut Akgul, Naoto Tokuyama, Xavier Farré, Robin Elliott, Vidya S Viswanathan, Holly Harper, Gregory MacLennan, Anant Madabhushi
{"title":"Computational Morphological Assessment of Bladder Cancer Tissue Is Prognostic of Recurrence and Overall Survival Following Transurethral Resection.","authors":"Patrick Leo, Behtash G Nezami, Mahmut Akgul, Naoto Tokuyama, Xavier Farré, Robin Elliott, Vidya S Viswanathan, Holly Harper, Gregory MacLennan, Anant Madabhushi","doi":"10.1200/CCI-24-00304","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Current risk assessment tools for bladder cancer following transurethral resection of the bladder tumor (TURBT) depend on pathological examination of resected tissue, with the consequent intra- and inter-reviewer variability. Improved prognostic tools could enable increased monitoring and aggressive interventions for high-risk patients while reducing the frequency of invasive testing for low-risk patients.</p><p><strong>Methods: </strong>We present an automated tumor risk assessment method based on quantitative features of nuclear pleomorphism and polarity extracted from digitized hematoxylin and eosin slides and compared this model with pathologist grading. Our model, incorporating six features, was trained to estimate overall survival risk on n = 189 patients and validated for recurrence prognosis on an independent validation set of n = 151 patients.</p><p><strong>Results: </strong>The model had an accuracy of 0.73 (95% CI, 0.66 to 0.81) in identifying patients who would have recurrence within 5 years of surgery. Within the validation set was a consensus set of patients (n = 94) on which three pathologists independently assigned the same grade and a nonconsensus set (n = 57) where they did not. The model had similar performance in the consensus and nonconsensus set, with accuracies of 0.70 (95% CI, 0.61 to 0.80) and 0.78 (95% CI, 0.67 to 0.89), respectively, and was able to recapitulate pathologist scoring on the consensus set (accuracy = 0.76).</p><p><strong>Conclusion: </strong>The results of this study suggest the need to incorporate both computerized analysis and pathologist grading into post-TURBT treatment planning.</p>","PeriodicalId":51626,"journal":{"name":"JCO Clinical Cancer Informatics","volume":"9 ","pages":"e2400304"},"PeriodicalIF":2.8000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12303250/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCO Clinical Cancer Informatics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1200/CCI-24-00304","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/22 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Current risk assessment tools for bladder cancer following transurethral resection of the bladder tumor (TURBT) depend on pathological examination of resected tissue, with the consequent intra- and inter-reviewer variability. Improved prognostic tools could enable increased monitoring and aggressive interventions for high-risk patients while reducing the frequency of invasive testing for low-risk patients.
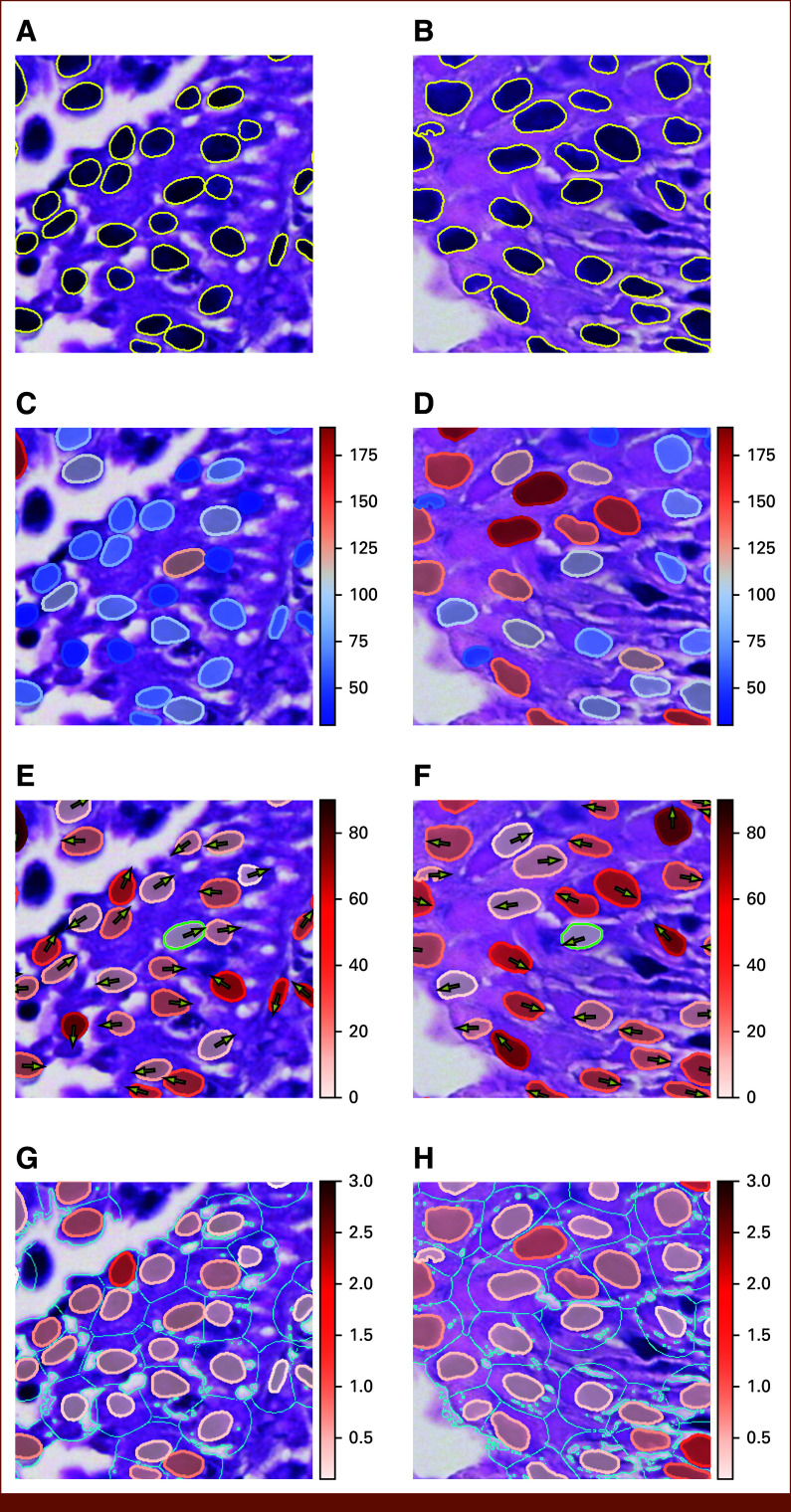
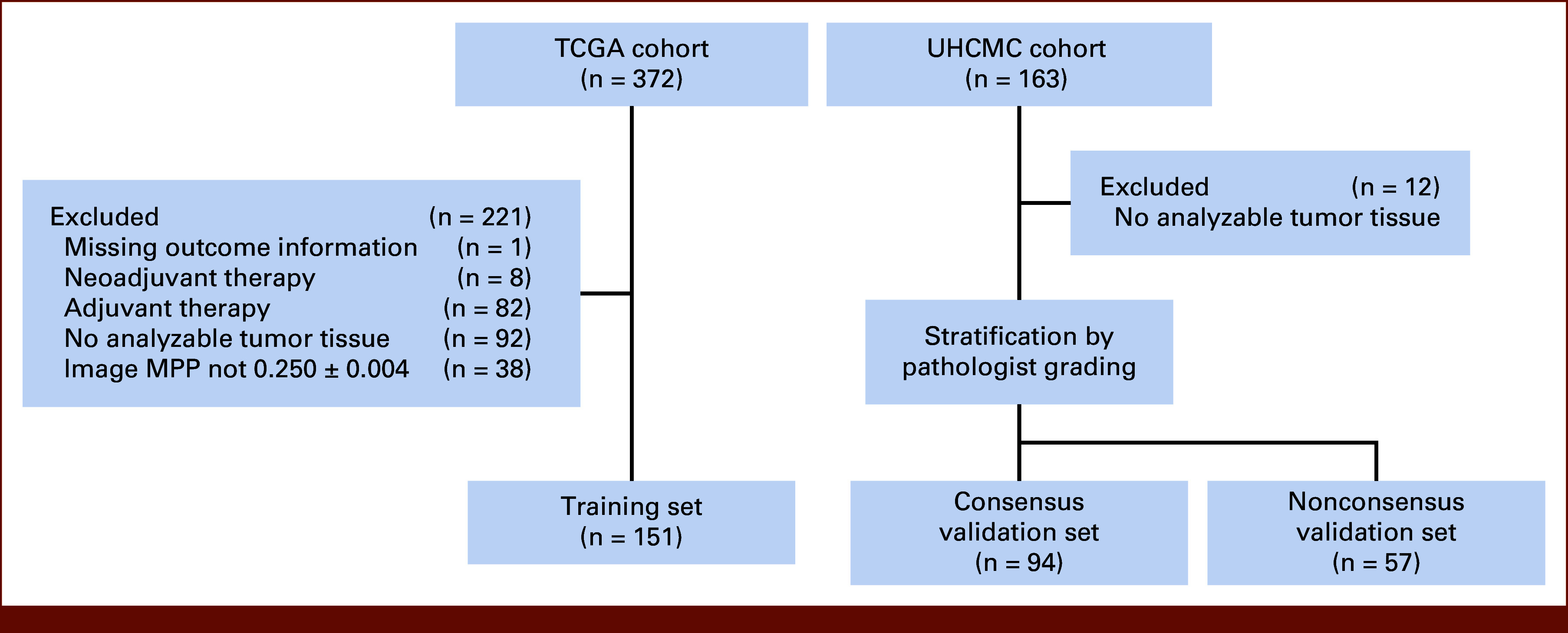
Methods: We present an automated tumor risk assessment method based on quantitative features of nuclear pleomorphism and polarity extracted from digitized hematoxylin and eosin slides and compared this model with pathologist grading. Our model, incorporating six features, was trained to estimate overall survival risk on n = 189 patients and validated for recurrence prognosis on an independent validation set of n = 151 patients.
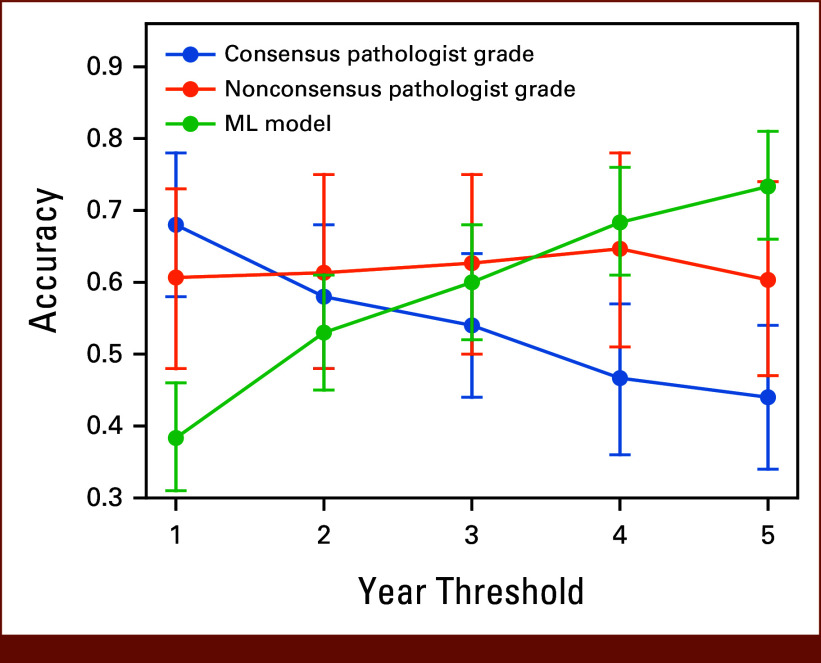
Results: The model had an accuracy of 0.73 (95% CI, 0.66 to 0.81) in identifying patients who would have recurrence within 5 years of surgery. Within the validation set was a consensus set of patients (n = 94) on which three pathologists independently assigned the same grade and a nonconsensus set (n = 57) where they did not. The model had similar performance in the consensus and nonconsensus set, with accuracies of 0.70 (95% CI, 0.61 to 0.80) and 0.78 (95% CI, 0.67 to 0.89), respectively, and was able to recapitulate pathologist scoring on the consensus set (accuracy = 0.76).
Conclusion: The results of this study suggest the need to incorporate both computerized analysis and pathologist grading into post-TURBT treatment planning.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


