{"title":"Observable score for bleeding after colorectal endoscopic mucosal resection.","authors":"Hayato Nakazawa, Kenichiro Okimoto, Tomoaki Matsumura, Masayuki Yokoyama, Tsubasa Ishikawa, Yoshihiro Fukuda, Yoshio Kitsukawa, Akane Kurosugi, Michiko Sonoda, Tatsuya Kaneko, Yuki Ohta, Takashi Taida, Keisuke Matsusaka, Jun-Ichiro Ikeda, Jun Kato","doi":"10.1177/17562848251356112","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is insufficient evidence regarding the management of hematochezia after colorectal endoscopic mucosal resection (EMR) without endoscopic hemostasis.</p><p><strong>Objectives: </strong>The aim of this study was to develop an observable score for hematochezia after colorectal EMR.</p><p><strong>Design: </strong>Retrospective study.</p><p><strong>Methods: </strong>This retrospective study included three hospitals in Japan. During the study period, colorectal EMR was performed in 3989 patients (11,414 lesions). Post-EMR hematochezia (delayed bleeding (DB)) was observed in 169 patients (512 lesions). Of these, 47 patients (150 lesions) were classified into the Hemostasis Group, comprising those who underwent endoscopic hemostasis. The remaining 122 (362 lesions) were classified into the non-hemostasis group, comprising those who underwent endoscopy without hemostasis, received preventive hemostasis, and did not undergo emergency endoscopy. Weighted points were assigned to predict observable cases following colorectal EMR through multivariate logistic regression analysis, enabling the development of a predictive model.</p><p><strong>Results: </strong>The prediction model comprised three variables (male gender, American Society of Anesthesiologists Physical Status 3, direct oral anticoagulant). According to the definition, the total score was categorized as lowly observable (2 or 3 points) and highly observable (0 or 1 points) for DB after colorectal EMR. As a result, the rates of observable cases for each risk category were 45.7% and 81.8%, respectively. The model showed good discrimination ability from the c-statistic (95% CI) of 0.71 (0.63-0.79).</p><p><strong>Conclusion: </strong>Although further prospective studies are necessary to validate the utility of the score, it may be useful in clinical practice.</p>","PeriodicalId":48770,"journal":{"name":"Therapeutic Advances in Gastroenterology","volume":"18 ","pages":"17562848251356112"},"PeriodicalIF":3.4000,"publicationDate":"2025-07-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12280549/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562848251356112","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: There is insufficient evidence regarding the management of hematochezia after colorectal endoscopic mucosal resection (EMR) without endoscopic hemostasis.
Objectives: The aim of this study was to develop an observable score for hematochezia after colorectal EMR.
Design: Retrospective study.
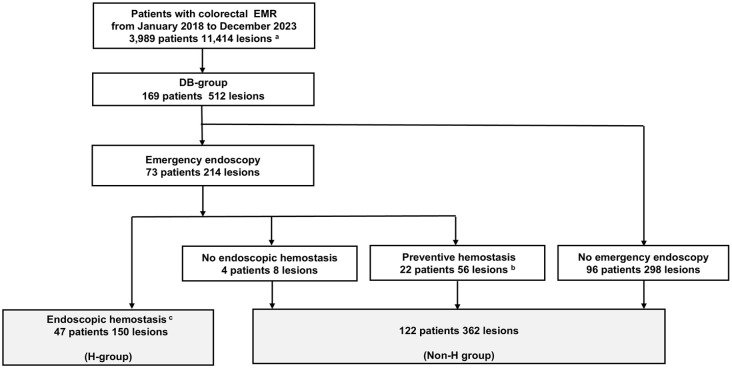
Methods: This retrospective study included three hospitals in Japan. During the study period, colorectal EMR was performed in 3989 patients (11,414 lesions). Post-EMR hematochezia (delayed bleeding (DB)) was observed in 169 patients (512 lesions). Of these, 47 patients (150 lesions) were classified into the Hemostasis Group, comprising those who underwent endoscopic hemostasis. The remaining 122 (362 lesions) were classified into the non-hemostasis group, comprising those who underwent endoscopy without hemostasis, received preventive hemostasis, and did not undergo emergency endoscopy. Weighted points were assigned to predict observable cases following colorectal EMR through multivariate logistic regression analysis, enabling the development of a predictive model.
Results: The prediction model comprised three variables (male gender, American Society of Anesthesiologists Physical Status 3, direct oral anticoagulant). According to the definition, the total score was categorized as lowly observable (2 or 3 points) and highly observable (0 or 1 points) for DB after colorectal EMR. As a result, the rates of observable cases for each risk category were 45.7% and 81.8%, respectively. The model showed good discrimination ability from the c-statistic (95% CI) of 0.71 (0.63-0.79).
Conclusion: Although further prospective studies are necessary to validate the utility of the score, it may be useful in clinical practice.
期刊介绍:
Therapeutic Advances in Gastroenterology is an open access journal which delivers the highest quality peer-reviewed original research articles, reviews, and scholarly comment on pioneering efforts and innovative studies in the medical treatment of gastrointestinal and hepatic disorders. The journal has a strong clinical and pharmacological focus and is aimed at an international audience of clinicians and researchers in gastroenterology and related disciplines, providing an online forum for rapid dissemination of recent research and perspectives in this area.
The editors welcome original research articles across all areas of gastroenterology and hepatology.
The journal publishes original research articles and review articles primarily. Original research manuscripts may include laboratory, animal or human/clinical studies – all phases. Letters to the Editor and Case Reports will also be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


