{"title":"Risk factors for pulmonary infection after thoracoscopic radical resection of lung cancer in elderly patients with diabetes mellitus.","authors":"Zi-Yuan Chen, Zhi-Qi Hong, Tie-Qiao Wang, Guo-Mei-Zhi Fu, Wen-Min Su, Cheng-Wei Zhou","doi":"10.4239/wjd.v16.i7.106903","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Lung cancer (LC) is one of the most prevalent cancers globally, with a high incidence among the elderly population. Elderly patients, particularly those with diabetes mellitus, are at an increased risk of postoperative complications, including pulmonary infections, due to weakened immune function and metabolic abnormalities. Postoperative pulmonary infection (PPI) is a predominant complication after thoracoscopic radical resection of LC, significantly affecting patient outcomes and increasing healthcare burdens. Determining risk factors for PPI in this vulnerable population is crucial for improving surgical outcomes and reducing infection rates.</p><p><strong>Aim: </strong>To develop and validate a predictive model for PPI in elderly patients with diabetes undergoing thoracoscopic radical resection for LC and to assess its reliability and validity.</p><p><strong>Methods: </strong>This retrospective study included 212 patients with LC who received treatment at our hospital from March 2015 to March 2022. General clinical information, surgical treatment details, and laboratory test results were collected and analyzed. Patients were grouped according to infection occurrence during the postoperative hospitalization period. Risk factors for PPIs were determined through logistic regression analysis, and a nomogram prediction model was established using R software to assess its predictive accuracy and performance.</p><p><strong>Results: </strong>Among the 212 patients [median age: 72 years (interquartile range: 60-82 years)], 41 developed PPI (19.34%), with Gram-negative bacteria being the predominant pathogens (64.14%). Factors, such as age of ≥ 70 years, presence of respiratory diseases, maximum tumor diameter of ≥ 4 cm, stages II-III, receiving neoadjuvant chemotherapy of ≥ 2 times preoperatively, surgery duration of ≥ 3 hours, chest drainage tube placement duration of ≥ 3.5 days, preoperative fasting blood glucose levels, hemoglobin A1c (HbA1c) levels, and multi-leaf resection, were markedly higher in the infection group than in the non-infection group. Conversely, forced expiratory volume in 1 second (FEV1) of ≥ 80% and albumin (Alb) levels were lower in the infection group. Multivariate logistic regression analysis revealed that receiving neoadjuvant chemotherapy of ≥ 2 times [odds ratio (OR) = 2.987; <i>P</i> = 0.036], maximum tumor diameter of ≥ 4 cm (OR = 3.959; <i>P</i> = 0.013), multi-leaf resection (OR = 3.18; <i>P</i> = 0.036), preoperative FEV1 of ≤ 80% (OR = 3.305; <i>P</i> = 0.029), and high HbA1c levels (OR = 2.39; <i>P</i> = 0.003) as key risk factors for PPI, whereas high Alb levels (OR = 0.507; <i>P</i> < 0.001) was protective. The nomogram model demonstrated excellent diagnostic ability (area under the curve = 0.901, 0.915), and calibration curves and decision curve analysis revealed good predictive performance and clinical applicability of the model.</p><p><strong>Conclusion: </strong>The primary pathogens of PPI in elderly patients with diabetes and LC undergoing thoracoscopic radical resection are Gram-negative bacteria. The nomogram model, based on preoperative neoadjuvant chemotherapy cycles, maximum tumor diameter, range of resection, and preoperative FEV1, Alb, and HbA1c levels, shows high clinical value in predicting the risk of PPI in this patient population.</p>","PeriodicalId":48607,"journal":{"name":"World Journal of Diabetes","volume":"16 7","pages":"106903"},"PeriodicalIF":4.6000,"publicationDate":"2025-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12278080/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Diabetes","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4239/wjd.v16.i7.106903","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Lung cancer (LC) is one of the most prevalent cancers globally, with a high incidence among the elderly population. Elderly patients, particularly those with diabetes mellitus, are at an increased risk of postoperative complications, including pulmonary infections, due to weakened immune function and metabolic abnormalities. Postoperative pulmonary infection (PPI) is a predominant complication after thoracoscopic radical resection of LC, significantly affecting patient outcomes and increasing healthcare burdens. Determining risk factors for PPI in this vulnerable population is crucial for improving surgical outcomes and reducing infection rates.
Aim: To develop and validate a predictive model for PPI in elderly patients with diabetes undergoing thoracoscopic radical resection for LC and to assess its reliability and validity.
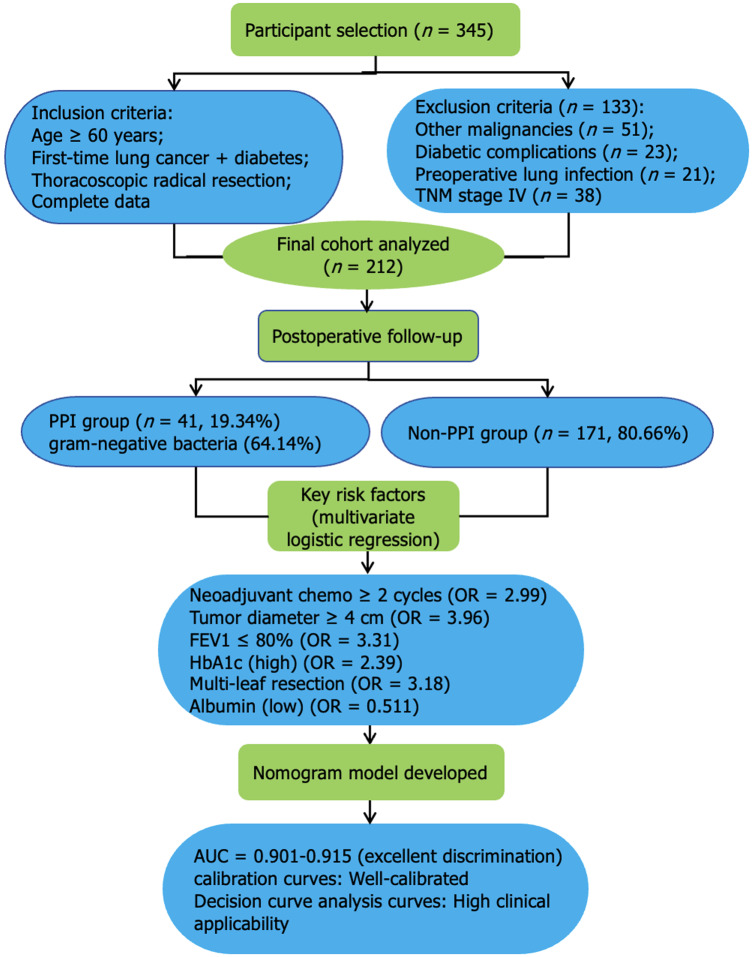
Methods: This retrospective study included 212 patients with LC who received treatment at our hospital from March 2015 to March 2022. General clinical information, surgical treatment details, and laboratory test results were collected and analyzed. Patients were grouped according to infection occurrence during the postoperative hospitalization period. Risk factors for PPIs were determined through logistic regression analysis, and a nomogram prediction model was established using R software to assess its predictive accuracy and performance.
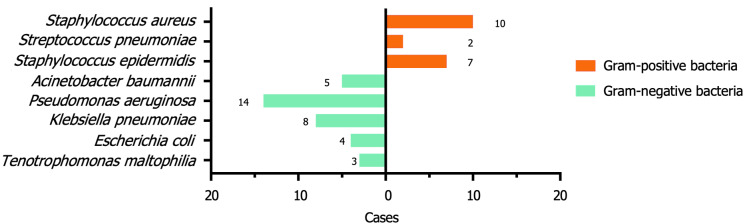
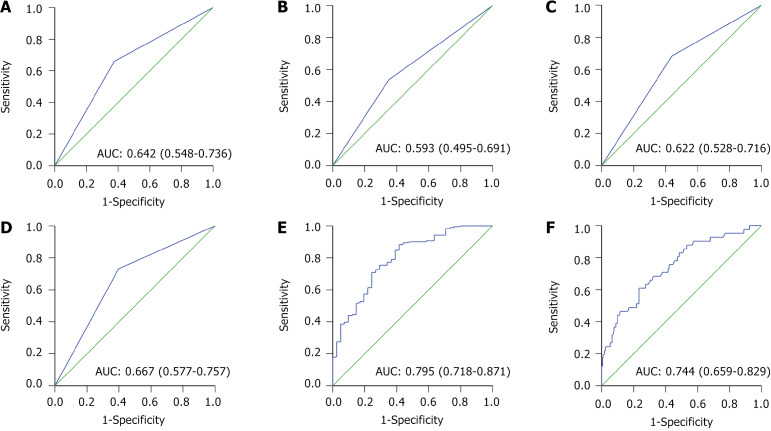
Results: Among the 212 patients [median age: 72 years (interquartile range: 60-82 years)], 41 developed PPI (19.34%), with Gram-negative bacteria being the predominant pathogens (64.14%). Factors, such as age of ≥ 70 years, presence of respiratory diseases, maximum tumor diameter of ≥ 4 cm, stages II-III, receiving neoadjuvant chemotherapy of ≥ 2 times preoperatively, surgery duration of ≥ 3 hours, chest drainage tube placement duration of ≥ 3.5 days, preoperative fasting blood glucose levels, hemoglobin A1c (HbA1c) levels, and multi-leaf resection, were markedly higher in the infection group than in the non-infection group. Conversely, forced expiratory volume in 1 second (FEV1) of ≥ 80% and albumin (Alb) levels were lower in the infection group. Multivariate logistic regression analysis revealed that receiving neoadjuvant chemotherapy of ≥ 2 times [odds ratio (OR) = 2.987; P = 0.036], maximum tumor diameter of ≥ 4 cm (OR = 3.959; P = 0.013), multi-leaf resection (OR = 3.18; P = 0.036), preoperative FEV1 of ≤ 80% (OR = 3.305; P = 0.029), and high HbA1c levels (OR = 2.39; P = 0.003) as key risk factors for PPI, whereas high Alb levels (OR = 0.507; P < 0.001) was protective. The nomogram model demonstrated excellent diagnostic ability (area under the curve = 0.901, 0.915), and calibration curves and decision curve analysis revealed good predictive performance and clinical applicability of the model.
Conclusion: The primary pathogens of PPI in elderly patients with diabetes and LC undergoing thoracoscopic radical resection are Gram-negative bacteria. The nomogram model, based on preoperative neoadjuvant chemotherapy cycles, maximum tumor diameter, range of resection, and preoperative FEV1, Alb, and HbA1c levels, shows high clinical value in predicting the risk of PPI in this patient population.
期刊介绍:
The WJD is a high-quality, peer reviewed, open-access journal. The primary task of WJD is to rapidly publish high-quality original articles, reviews, editorials, and case reports in the field of diabetes. In order to promote productive academic communication, the peer review process for the WJD is transparent; to this end, all published manuscripts are accompanied by the anonymized reviewers’ comments as well as the authors’ responses. The primary aims of the WJD are to improve diagnostic, therapeutic and preventive modalities and the skills of clinicians and to guide clinical practice in diabetes. Scope: Diabetes Complications, Experimental Diabetes Mellitus, Type 1 Diabetes Mellitus, Type 2 Diabetes Mellitus, Diabetes, Gestational, Diabetic Angiopathies, Diabetic Cardiomyopathies, Diabetic Coma, Diabetic Ketoacidosis, Diabetic Nephropathies, Diabetic Neuropathies, Donohue Syndrome, Fetal Macrosomia, and Prediabetic State.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


