{"title":"Predictive model and risk analysis for outcomes in diabetic foot ulcer using eXtreme Gradient Boosting algorithm and SHapley Additive exPlanation.","authors":"Lei Gao, Zi-Xuan Liu, Jiang-Ning Wang","doi":"10.4239/wjd.v16.i7.104789","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Diabetic foot ulcer (DFU) is a serious and destructive complication of diabetes, which has a high amputation rate and carries a huge social burden. Early detection of risk factors and intervention are essential to reduce amputation rates. With the development of artificial intelligence technology, efficient interpretable predictive models can be generated in clinical practice to improve DFU care.</p><p><strong>Aim: </strong>To develop and validate an interpretable model for predicting amputation risk in DFU patients.</p><p><strong>Methods: </strong>This retrospective study collected basic data from 599 patients with DFU in Beijing Shijitan Hospital between January 2015 and June 2024. The data set was randomly divided into a training set and test set with fivefold cross-validation. Three binary variable models were built with the eXtreme Gradient Boosting (XGBoost) algorithm to input risk factors that predict amputation probability. The model performance was optimized by adjusting the super parameters. The predictive performance of the three models was expressed by sensitivity, specificity, positive predictive value, negative predictive value and area under the curve (AUC). Visualization of the prediction results was realized through SHapley Additive exPlanation (SHAP).</p><p><strong>Results: </strong>A total of 157 (26.2%) patients underwent minor amputation during hospitalization and 50 (8.3%) had major amputation. All three XGBoost models demonstrated good discriminative ability, with AUC values > 0.7. The model for predicting major amputation achieved the highest performance [AUC = 0.977, 95% confidence interval (CI): 0.956-0.998], followed by the minor amputation model (AUC = 0.800, 95%CI: 0.762-0.838) and the non-amputation model (AUC = 0.772, 95%CI: 0.730-0.814). Feature importance ranking of the three models revealed the risk factors for minor and major amputation. Wagner grade 4/5, osteomyelitis, and high C-reactive protein were all considered important predictive variables.</p><p><strong>Conclusion: </strong>XGBoost effectively predicts diabetic foot amputation risk and provides interpretable insights to support personalized treatment decisions.</p>","PeriodicalId":48607,"journal":{"name":"World Journal of Diabetes","volume":"16 7","pages":"104789"},"PeriodicalIF":4.6000,"publicationDate":"2025-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12278075/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Diabetes","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4239/wjd.v16.i7.104789","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Diabetic foot ulcer (DFU) is a serious and destructive complication of diabetes, which has a high amputation rate and carries a huge social burden. Early detection of risk factors and intervention are essential to reduce amputation rates. With the development of artificial intelligence technology, efficient interpretable predictive models can be generated in clinical practice to improve DFU care.
Aim: To develop and validate an interpretable model for predicting amputation risk in DFU patients.
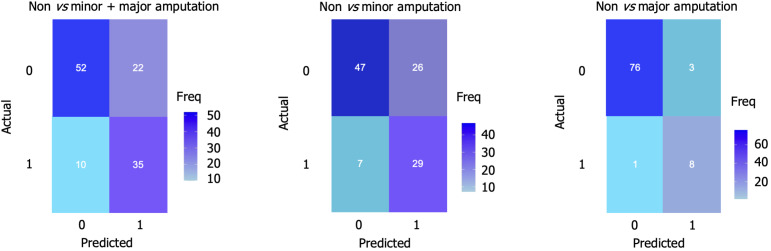
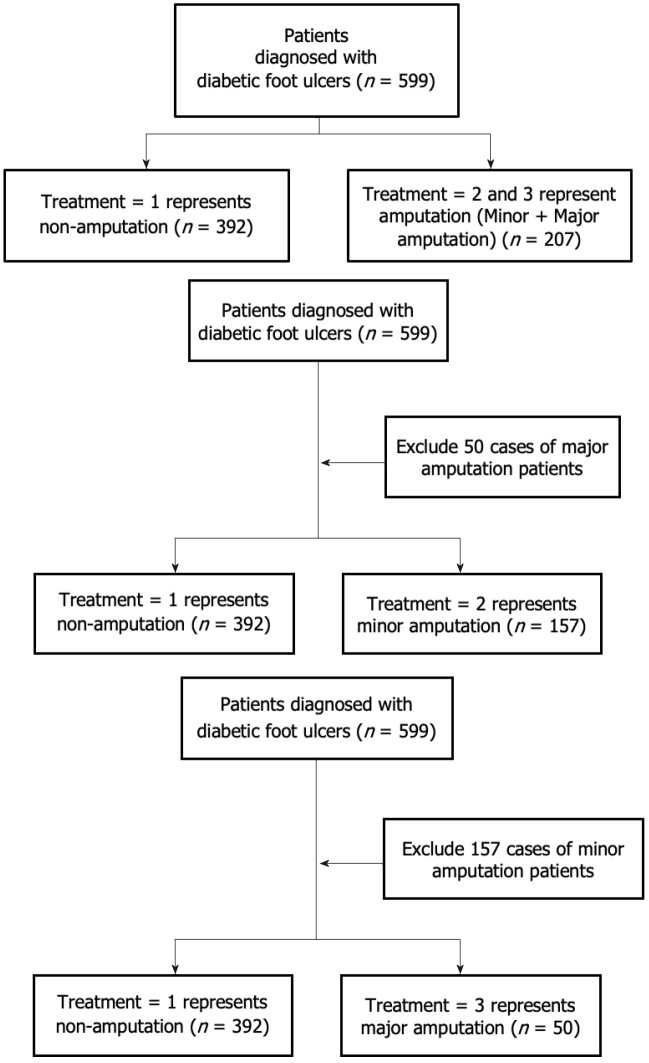
Methods: This retrospective study collected basic data from 599 patients with DFU in Beijing Shijitan Hospital between January 2015 and June 2024. The data set was randomly divided into a training set and test set with fivefold cross-validation. Three binary variable models were built with the eXtreme Gradient Boosting (XGBoost) algorithm to input risk factors that predict amputation probability. The model performance was optimized by adjusting the super parameters. The predictive performance of the three models was expressed by sensitivity, specificity, positive predictive value, negative predictive value and area under the curve (AUC). Visualization of the prediction results was realized through SHapley Additive exPlanation (SHAP).
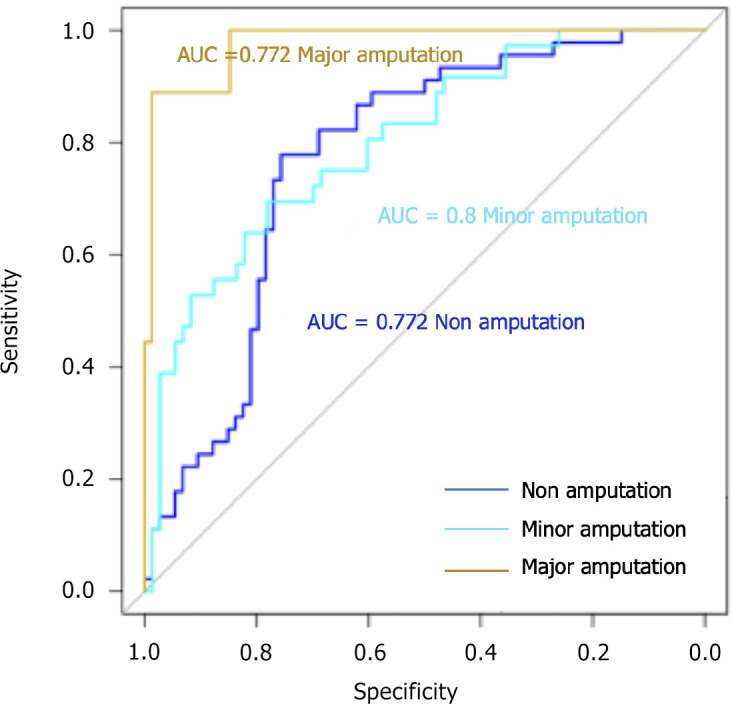
Results: A total of 157 (26.2%) patients underwent minor amputation during hospitalization and 50 (8.3%) had major amputation. All three XGBoost models demonstrated good discriminative ability, with AUC values > 0.7. The model for predicting major amputation achieved the highest performance [AUC = 0.977, 95% confidence interval (CI): 0.956-0.998], followed by the minor amputation model (AUC = 0.800, 95%CI: 0.762-0.838) and the non-amputation model (AUC = 0.772, 95%CI: 0.730-0.814). Feature importance ranking of the three models revealed the risk factors for minor and major amputation. Wagner grade 4/5, osteomyelitis, and high C-reactive protein were all considered important predictive variables.
Conclusion: XGBoost effectively predicts diabetic foot amputation risk and provides interpretable insights to support personalized treatment decisions.
期刊介绍:
The WJD is a high-quality, peer reviewed, open-access journal. The primary task of WJD is to rapidly publish high-quality original articles, reviews, editorials, and case reports in the field of diabetes. In order to promote productive academic communication, the peer review process for the WJD is transparent; to this end, all published manuscripts are accompanied by the anonymized reviewers’ comments as well as the authors’ responses. The primary aims of the WJD are to improve diagnostic, therapeutic and preventive modalities and the skills of clinicians and to guide clinical practice in diabetes. Scope: Diabetes Complications, Experimental Diabetes Mellitus, Type 1 Diabetes Mellitus, Type 2 Diabetes Mellitus, Diabetes, Gestational, Diabetic Angiopathies, Diabetic Cardiomyopathies, Diabetic Coma, Diabetic Ketoacidosis, Diabetic Nephropathies, Diabetic Neuropathies, Donohue Syndrome, Fetal Macrosomia, and Prediabetic State.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


