Madeline B Thomas, Sumaya Abdul Ghaffar, Haaris Kadri, Christopher M Quinn, Laura D Leonard, Nicole M Mott, Salvador Rodriguez Franco, Lia R Assumpção, Gretchen Ahrendt, Sarah E A Tevis, Nicole Christian, Jodi Widner, Alicia A Heelan, Ana L Gleisner
{"title":"Multi-level factors drive use of sentinel lymph node biopsy in older women with early-stage breast cancer.","authors":"Madeline B Thomas, Sumaya Abdul Ghaffar, Haaris Kadri, Christopher M Quinn, Laura D Leonard, Nicole M Mott, Salvador Rodriguez Franco, Lia R Assumpção, Gretchen Ahrendt, Sarah E A Tevis, Nicole Christian, Jodi Widner, Alicia A Heelan, Ana L Gleisner","doi":"10.1007/s10549-025-07789-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>In 2016, the Society of Surgical Oncology and Choosing Wisely Campaign recommended against sentinel lymph node biopsy (SLNB) in women > 70 years with early-stage, hormone receptor-positive (ER/PR +) breast cancer, citing limited clinical benefit. Despite earlier evidence supporting de-implementation, SLNB rates remained high. We aimed to evaluate patient, tumor, facility, and unmeasured contextual factors associated with SLNB de-implementation using a national cohort.</p><p><strong>Methods: </strong>We queried the National Cancer Database (NCDB) for women > 70 years diagnosed with early-stage ER/PR + and HER2-negative breast cancer between 2012 and 2019. A mixed effects logistic regression model assessed associations between SLNB non-utilization and patient, tumor, and facility-level characteristics. Interaction terms between year and facility breast surgery volume quartiles were included to examine trends over time. Reference Effect Measures (REM) were used to estimate the contribution of unmeasured contextual effects relative to measured covariates.</p><p><strong>Results: </strong>Among eligible patients, SLNB use declined from 86.7% in 2012 to 81.0% in 2019. SLNB use was significantly associated with age, insurance, urbanization, distance to facility, education, income, tumor size, lymphovascular invasion, treatment type, facility region, program type, and surgical volume. Academic programs had the highest adjusted odds of SLNB non-utilization (AOR 1.62; 95%CI: 1.29-2.02), while facilities in the South had the lowest (AOR 0.53; 95%CI: 0.45-0.63). High-volume centers de-implemented more rapidly post-2016, with 24% higher odds of SLNB non-utilization per year. REM analysis identified patient age and unmeasured contextual effects as the predominant drivers of de-implementation.</p><p><strong>Conclusion: </strong>SLNB use in older women is influenced by multi-level factors, with patient age and unmeasured contextual effects driving de-implementation-though progress remain slow and limited in the United States.</p>","PeriodicalId":9133,"journal":{"name":"Breast Cancer Research and Treatment","volume":" ","pages":"37-48"},"PeriodicalIF":3.0000,"publicationDate":"2025-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12398473/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Breast Cancer Research and Treatment","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10549-025-07789-1","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/22 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: In 2016, the Society of Surgical Oncology and Choosing Wisely Campaign recommended against sentinel lymph node biopsy (SLNB) in women > 70 years with early-stage, hormone receptor-positive (ER/PR +) breast cancer, citing limited clinical benefit. Despite earlier evidence supporting de-implementation, SLNB rates remained high. We aimed to evaluate patient, tumor, facility, and unmeasured contextual factors associated with SLNB de-implementation using a national cohort.
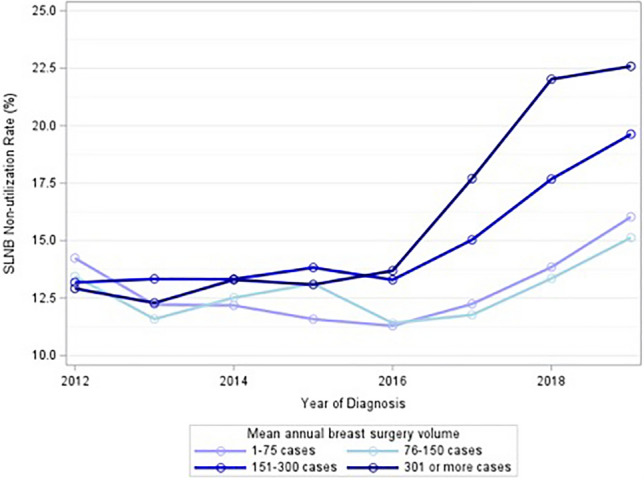
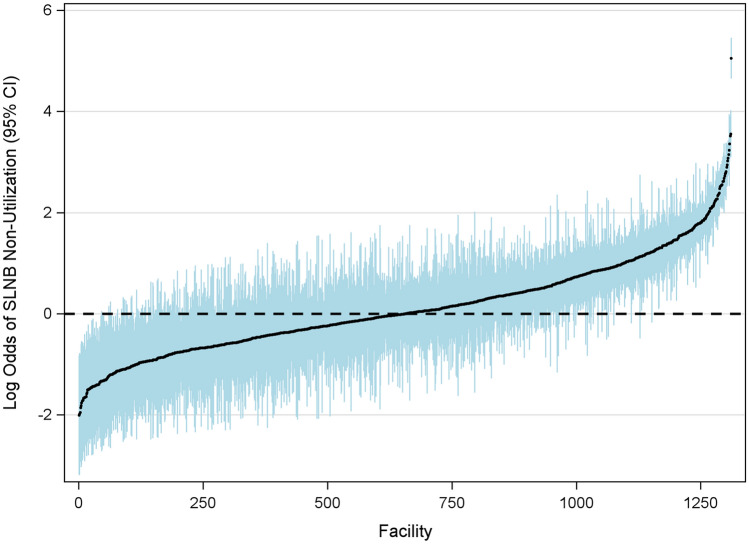
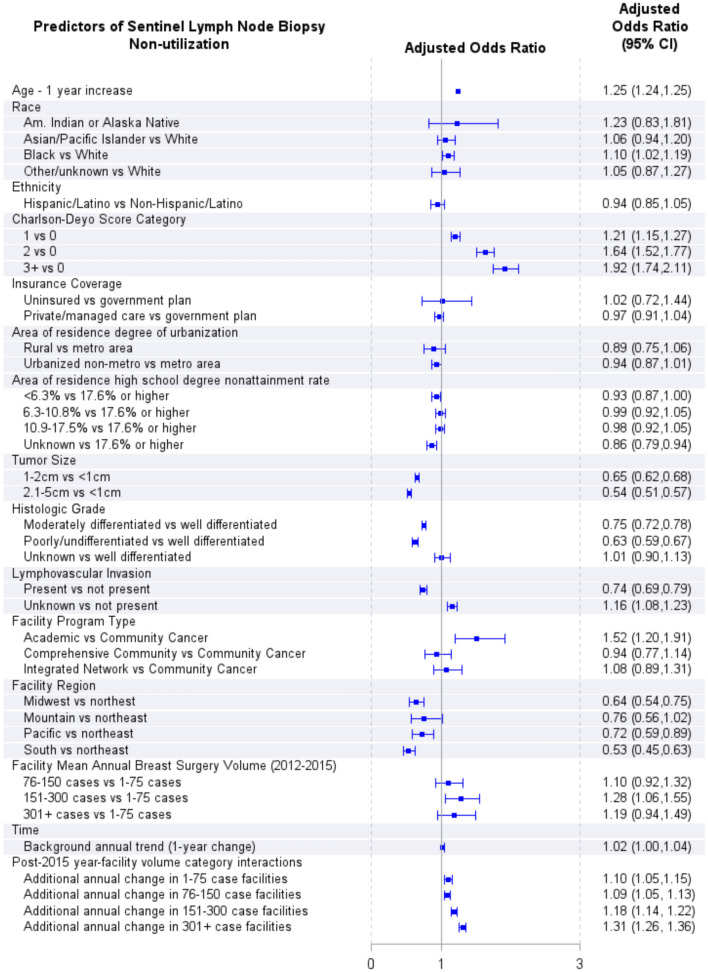
Methods: We queried the National Cancer Database (NCDB) for women > 70 years diagnosed with early-stage ER/PR + and HER2-negative breast cancer between 2012 and 2019. A mixed effects logistic regression model assessed associations between SLNB non-utilization and patient, tumor, and facility-level characteristics. Interaction terms between year and facility breast surgery volume quartiles were included to examine trends over time. Reference Effect Measures (REM) were used to estimate the contribution of unmeasured contextual effects relative to measured covariates.
Results: Among eligible patients, SLNB use declined from 86.7% in 2012 to 81.0% in 2019. SLNB use was significantly associated with age, insurance, urbanization, distance to facility, education, income, tumor size, lymphovascular invasion, treatment type, facility region, program type, and surgical volume. Academic programs had the highest adjusted odds of SLNB non-utilization (AOR 1.62; 95%CI: 1.29-2.02), while facilities in the South had the lowest (AOR 0.53; 95%CI: 0.45-0.63). High-volume centers de-implemented more rapidly post-2016, with 24% higher odds of SLNB non-utilization per year. REM analysis identified patient age and unmeasured contextual effects as the predominant drivers of de-implementation.
Conclusion: SLNB use in older women is influenced by multi-level factors, with patient age and unmeasured contextual effects driving de-implementation-though progress remain slow and limited in the United States.
期刊介绍:
Breast Cancer Research and Treatment provides the surgeon, radiotherapist, medical oncologist, endocrinologist, epidemiologist, immunologist or cell biologist investigating problems in breast cancer a single forum for communication. The journal creates a "market place" for breast cancer topics which cuts across all the usual lines of disciplines, providing a site for presenting pertinent investigations, and for discussing critical questions relevant to the entire field. It seeks to develop a new focus and new perspectives for all those concerned with breast cancer.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


