{"title":"Diagnostic model for COPD patients with nocardia infection: a study based on clinical features and risk factors.","authors":"Kai Zhang, Kangli Yang, Hongmin Wang","doi":"10.1177/17534666251359139","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The escalating morbidity and mortality of chronic obstructive pulmonary disease (COPD) necessitates improved diagnostic approaches for comorbid infections. COPD patients exhibit heightened susceptibility to opportunistic pathogens like Nocardia species due to compromised airway defenses and frequent glucocorticoid/immuno-suppressant use. Despite its clinical significance, Nocardia infection remains diagnostically challenging due to nonspecific presentations and imaging features.</p><p><strong>Objectives: </strong>To develop and validate a diagnostic model integrating clinical characteristics and risk factors for COPD complicated by Nocardia infection.</p><p><strong>Design: </strong>A retrospective analysis was conducted on clinical data from 586 patients diagnosed with COPD and Nocardia infection, including clinical symptoms, laboratory tests, imaging findings, and treatment outcomes. Patients were screened according to inclusion and exclusion criteria and divided into two groups: COPD with Nocardia infection group (infection group) and COPD-only group (control group).</p><p><strong>Methods: </strong>This retrospective study analyzed 586 COPD patients (2019-2024), stratified into Nocardia-infected (<i>n</i> = 289) and noninfected (<i>n</i> = 297) cohorts. Demographic, laboratory, pulmonary function, and imaging data were collected. Multivariate logistic regression identified independent predictors, which informed a nomogram model. Model performance was assessed via concordance index (C-index), calibration curves, and ROC analysis.</p><p><strong>Results: </strong>Independent risk factors included hemoptysis (OR = 1.99, 95% CI: 0.76-5.26), lymphocyte count (OR = 6.81, 95% CI: 4.06-11.42), hemoglobin (OR = 1.01, 95% CI: 0.99-1.03), and pulmonary function parameters (FEV₁/FVC ratio OR = 12.47, 95% CI: 1.25-124.16). The model demonstrated excellent discrimination (C-index: 0.895 infected, 0.829 noninfected) and calibration (mean absolute error: 0.127-0.170). ROC analysis revealed AUCs of 0.896 (95% CI: 0.90-0.97) and 0.830 (95% CI: 0.77-0.89) for infected and noninfected groups, respectively.</p><p><strong>Conclusion: </strong>This validated nomogram provides a clinically actionable tool for early Nocardia detection in COPD patients, addressing a critical diagnostic gap. External validation is warranted to confirm generalizability.</p>","PeriodicalId":22884,"journal":{"name":"Therapeutic Advances in Respiratory Disease","volume":"19 ","pages":"17534666251359139"},"PeriodicalIF":3.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12280267/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Respiratory Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17534666251359139","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/21 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The escalating morbidity and mortality of chronic obstructive pulmonary disease (COPD) necessitates improved diagnostic approaches for comorbid infections. COPD patients exhibit heightened susceptibility to opportunistic pathogens like Nocardia species due to compromised airway defenses and frequent glucocorticoid/immuno-suppressant use. Despite its clinical significance, Nocardia infection remains diagnostically challenging due to nonspecific presentations and imaging features.
Objectives: To develop and validate a diagnostic model integrating clinical characteristics and risk factors for COPD complicated by Nocardia infection.
Design: A retrospective analysis was conducted on clinical data from 586 patients diagnosed with COPD and Nocardia infection, including clinical symptoms, laboratory tests, imaging findings, and treatment outcomes. Patients were screened according to inclusion and exclusion criteria and divided into two groups: COPD with Nocardia infection group (infection group) and COPD-only group (control group).
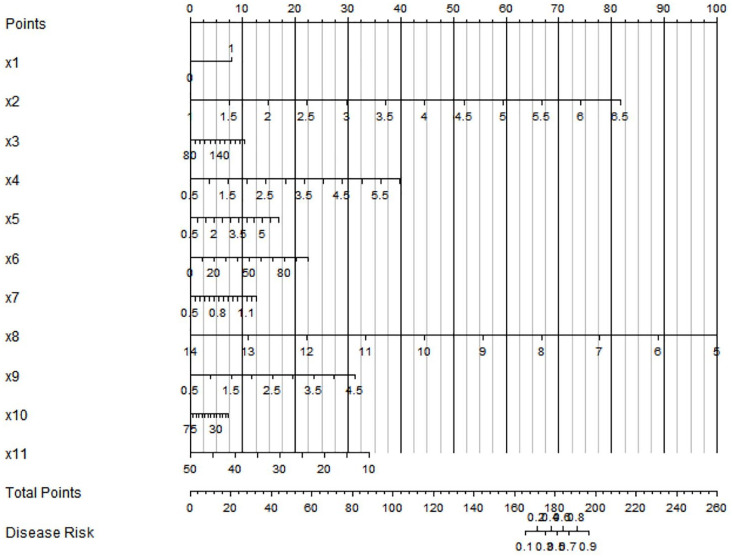
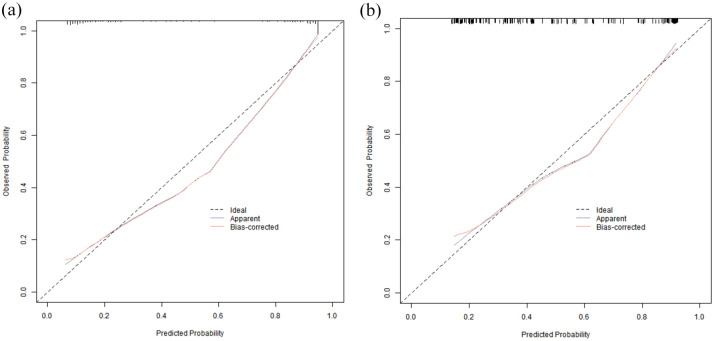
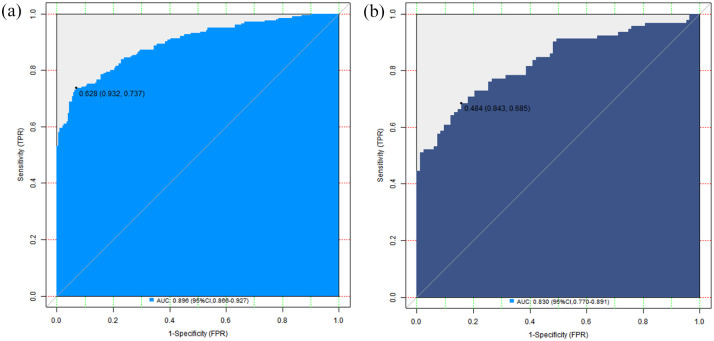
Methods: This retrospective study analyzed 586 COPD patients (2019-2024), stratified into Nocardia-infected (n = 289) and noninfected (n = 297) cohorts. Demographic, laboratory, pulmonary function, and imaging data were collected. Multivariate logistic regression identified independent predictors, which informed a nomogram model. Model performance was assessed via concordance index (C-index), calibration curves, and ROC analysis.
Results: Independent risk factors included hemoptysis (OR = 1.99, 95% CI: 0.76-5.26), lymphocyte count (OR = 6.81, 95% CI: 4.06-11.42), hemoglobin (OR = 1.01, 95% CI: 0.99-1.03), and pulmonary function parameters (FEV₁/FVC ratio OR = 12.47, 95% CI: 1.25-124.16). The model demonstrated excellent discrimination (C-index: 0.895 infected, 0.829 noninfected) and calibration (mean absolute error: 0.127-0.170). ROC analysis revealed AUCs of 0.896 (95% CI: 0.90-0.97) and 0.830 (95% CI: 0.77-0.89) for infected and noninfected groups, respectively.
Conclusion: This validated nomogram provides a clinically actionable tool for early Nocardia detection in COPD patients, addressing a critical diagnostic gap. External validation is warranted to confirm generalizability.
期刊介绍:
Therapeutic Advances in Respiratory Disease delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of respiratory disease.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


