Eseosa Grace Igbinosa, Bodini Dharmasekara, Jennifer K Quint, Sanjay Popat, Krishnan Bhaskaran, Daniel Morganstein, Sarah Cook
{"title":"Mortality Outcomes in People with Lung Cancer with and without Type2 Diabetes: A Cohort Study in England.","authors":"Eseosa Grace Igbinosa, Bodini Dharmasekara, Jennifer K Quint, Sanjay Popat, Krishnan Bhaskaran, Daniel Morganstein, Sarah Cook","doi":"10.2147/CLEP.S498368","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The impact of type 2 diabetes (T2DM) on mortality following lung cancer diagnosis remains unclear, with conflicting evidence across studies. We aimed to assess differences in all-cause and cause-specific mortality between people with lung cancer with and without T2DM within a primary care population in England.</p><p><strong>Methods: </strong>The study population was 69,674 people with incident lung cancer within the Clinical Practice Research Datalink (CPRD) Aurum primary care database (2010-2022). The study exposure was T2DM at cancer diagnosis, and the outcomes were all-cause and cause-specific mortality (cancer, cardio-vascular, respiratory). Cox models were fitted for each outcome adjusting for age, gender, smoking status, body mass index, calendar year and socioeconomic status (Index of Multiple Deprivation).</p><p><strong>Results: </strong>After adjusting for age and gender, there was no evidence for a difference in all-cause mortality in people with T2DM compared with people without T2DM (IRR 0.98 95% CI 0.96, 1.01). After fully-adjusting for measured confounders, there was a small positive effect (IRR 1.07 95% CI 1.04, 1.09). After adjusting for age and gender, people with T2DM had lower rates of cancer-specific mortality compared to people without T2DM (IRR 0.96 95% CI 0.94, 0.98). However, after adjustment for all measured confounders there was a small positive association (IRR 1.05 95% CI 1.02, 1.07). In both age and gender adjusted and fully adjusted models people with T2DM had higher cardiovascular (fully adjusted HR 1.30 95% CI 1.15, 1.47) and respiratory disease mortality (fully adjusted HR 1.30 95% CI 1.15, 1.47).</p><p><strong>Conclusion: </strong>There was robust evidence that people with T2DM had higher cardiovascular and respiratory disease mortality following lung cancer diagnosis. The relationships between T2DM and all-cause and cancer-specific mortality were highly sensitive to adjustment for confounding. Differences in studies on approaches to confounding and levels of missing data may contribute to the mixed findings on this association in the literature.</p>","PeriodicalId":10362,"journal":{"name":"Clinical Epidemiology","volume":"17 ","pages":"681-692"},"PeriodicalIF":3.2000,"publicationDate":"2025-07-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12278945/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/CLEP.S498368","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The impact of type 2 diabetes (T2DM) on mortality following lung cancer diagnosis remains unclear, with conflicting evidence across studies. We aimed to assess differences in all-cause and cause-specific mortality between people with lung cancer with and without T2DM within a primary care population in England.
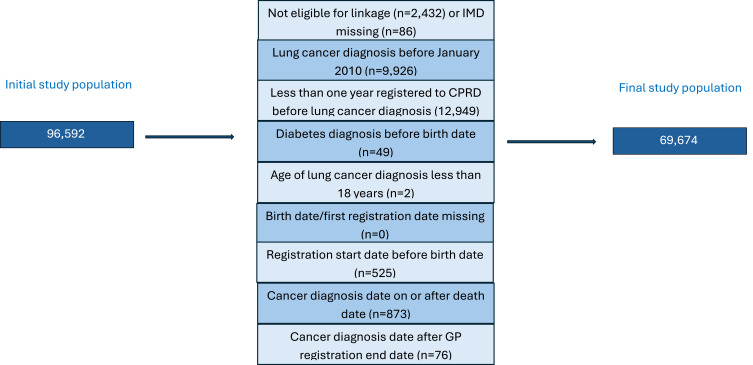
Methods: The study population was 69,674 people with incident lung cancer within the Clinical Practice Research Datalink (CPRD) Aurum primary care database (2010-2022). The study exposure was T2DM at cancer diagnosis, and the outcomes were all-cause and cause-specific mortality (cancer, cardio-vascular, respiratory). Cox models were fitted for each outcome adjusting for age, gender, smoking status, body mass index, calendar year and socioeconomic status (Index of Multiple Deprivation).
Results: After adjusting for age and gender, there was no evidence for a difference in all-cause mortality in people with T2DM compared with people without T2DM (IRR 0.98 95% CI 0.96, 1.01). After fully-adjusting for measured confounders, there was a small positive effect (IRR 1.07 95% CI 1.04, 1.09). After adjusting for age and gender, people with T2DM had lower rates of cancer-specific mortality compared to people without T2DM (IRR 0.96 95% CI 0.94, 0.98). However, after adjustment for all measured confounders there was a small positive association (IRR 1.05 95% CI 1.02, 1.07). In both age and gender adjusted and fully adjusted models people with T2DM had higher cardiovascular (fully adjusted HR 1.30 95% CI 1.15, 1.47) and respiratory disease mortality (fully adjusted HR 1.30 95% CI 1.15, 1.47).
Conclusion: There was robust evidence that people with T2DM had higher cardiovascular and respiratory disease mortality following lung cancer diagnosis. The relationships between T2DM and all-cause and cancer-specific mortality were highly sensitive to adjustment for confounding. Differences in studies on approaches to confounding and levels of missing data may contribute to the mixed findings on this association in the literature.
期刊介绍:
Clinical Epidemiology is an international, peer reviewed, open access journal. Clinical Epidemiology focuses on the application of epidemiological principles and questions relating to patients and clinical care in terms of prevention, diagnosis, prognosis, and treatment.
Clinical Epidemiology welcomes papers covering these topics in form of original research and systematic reviews.
Clinical Epidemiology has a special interest in international electronic medical patient records and other routine health care data, especially as applied to safety of medical interventions, clinical utility of diagnostic procedures, understanding short- and long-term clinical course of diseases, clinical epidemiological and biostatistical methods, and systematic reviews.
When considering submission of a paper utilizing publicly-available data, authors should ensure that such studies add significantly to the body of knowledge and that they use appropriate validated methods for identifying health outcomes.
The journal has launched special series describing existing data sources for clinical epidemiology, international health care systems and validation studies of algorithms based on databases and registries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


