{"title":"Adding Tolvaptan in the Inpatient Treatment for Patients with Heart Failure and Hyponatremia: Budget Impact Analysis in Thailand.","authors":"Unchalee Permsuwan, Krit Leemasawat, Poukwan Arunmanakul","doi":"10.2147/CEOR.S503735","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Tolvaptan is used as an add-on therapy for heart failure (HF) patients with volume overload, particularly those with hyponatremia (HN), but its cost raises concern. This study aimed to estimate the budget impact of adding 30 mg of tolvaptan to standard treatment compared to standard treatment alone in hospitalized HF patients with HN in Thailand.</p><p><strong>Methods: </strong>A budget impact analysis (BIA) model was developed in accordance with Thai Health Technology Assessment guidelines from the payer's perspective. Epidemiological data on HF in Thailand were used to estimate the target population. Clinical effectiveness data were derived from the EVEREST trial. Cost components included tolvaptan acquisition and HF-related hospitalization costs. Cost data were sourced from the National Health Security Office. The net budget impact (NBI) was calculated as the difference in total budget between standard care with tolvaptan and standard care alone. Deterministic sensitivity analysis was performed to explore the impact of key variables.</p><p><strong>Results: </strong>The total budget without tolvaptan was 201 million THB (5,802,973 USD), increasing to 221 million THB (6,365,607 USD) with tolvaptan, resulting in an NBI of 19.5 million THB (562,634 USD) or 1117 THB (32 USD) per member. Despite higher drug costs, tolvaptan use reduced hospitalization costs (4.2 million USD vs 5.8 million USD) due to fewer HF hospitalization days and length of stay reduction. A lower tolvaptan dose, reduced HN risk, or a daily cost reduction of at least 25.5% could result in a negative NBI.</p><p><strong>Conclusion: </strong>Although tolvaptan reduced hospital length of stay, its use at 30 mg daily still led to a positive NBI. These findings are relevant for Thailand and similar healthcare systems considering tolvaptan adoption.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"17 ","pages":"485-494"},"PeriodicalIF":2.2000,"publicationDate":"2025-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12276736/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S503735","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Tolvaptan is used as an add-on therapy for heart failure (HF) patients with volume overload, particularly those with hyponatremia (HN), but its cost raises concern. This study aimed to estimate the budget impact of adding 30 mg of tolvaptan to standard treatment compared to standard treatment alone in hospitalized HF patients with HN in Thailand.
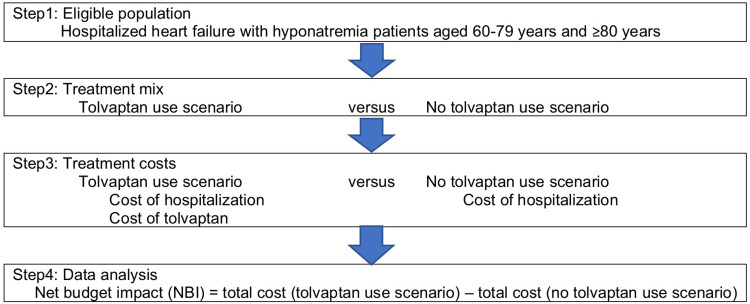
Methods: A budget impact analysis (BIA) model was developed in accordance with Thai Health Technology Assessment guidelines from the payer's perspective. Epidemiological data on HF in Thailand were used to estimate the target population. Clinical effectiveness data were derived from the EVEREST trial. Cost components included tolvaptan acquisition and HF-related hospitalization costs. Cost data were sourced from the National Health Security Office. The net budget impact (NBI) was calculated as the difference in total budget between standard care with tolvaptan and standard care alone. Deterministic sensitivity analysis was performed to explore the impact of key variables.
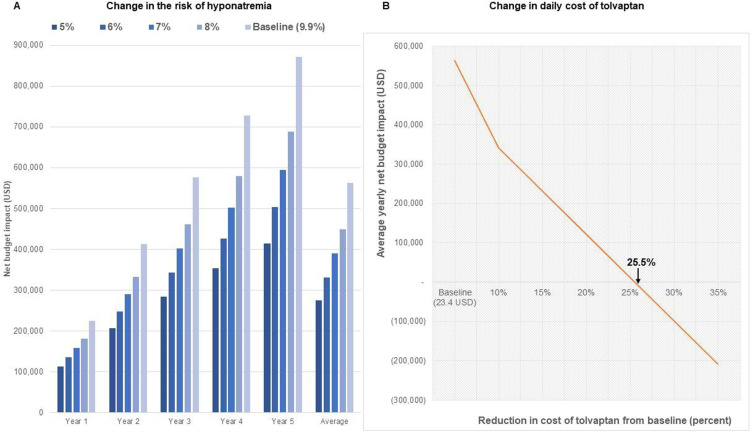
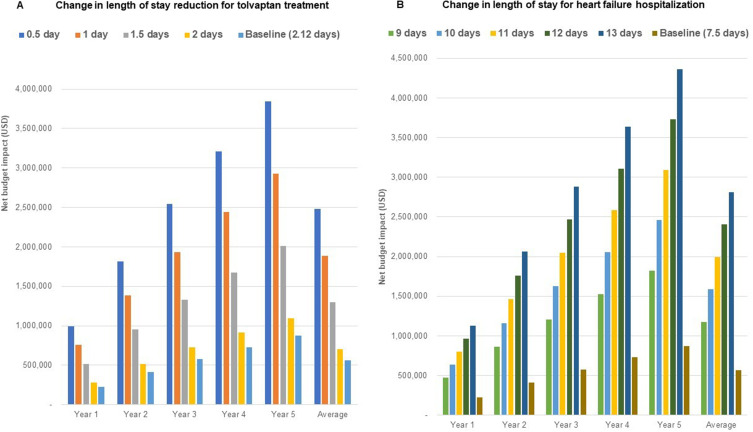
Results: The total budget without tolvaptan was 201 million THB (5,802,973 USD), increasing to 221 million THB (6,365,607 USD) with tolvaptan, resulting in an NBI of 19.5 million THB (562,634 USD) or 1117 THB (32 USD) per member. Despite higher drug costs, tolvaptan use reduced hospitalization costs (4.2 million USD vs 5.8 million USD) due to fewer HF hospitalization days and length of stay reduction. A lower tolvaptan dose, reduced HN risk, or a daily cost reduction of at least 25.5% could result in a negative NBI.
Conclusion: Although tolvaptan reduced hospital length of stay, its use at 30 mg daily still led to a positive NBI. These findings are relevant for Thailand and similar healthcare systems considering tolvaptan adoption.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


